Chapter 15. Adrenal Gland
(Atlas of Ultrasound)
1 Hemorrhage and Calcification
DESCRIPTION AND CLINICAL FEATURES
Neonatal adrenal hemorrhage may be seen in the setting of perinatal asphyxia and neonatal sepsis. Thus, adrenal hemorrhage in the fetus is thought to occur as a result of an in utero hypoxic insult. It is most often encountered in the third trimester. Often the timing and cause of the hypoxic injury is unknown. Adrenal hemorrhage may also occur as a complication of in utero renal vein thrombosis, likely because of altered flow to and from the adrenal gland in this condition.
Adrenal calcifications may be seen in the aftermath of an adrenal hemorrhage. They may also be encountered in the presence of some rare metabolic abnormalities, such as Wolman syndrome. Adrenal hemorrhage, especially if bilateral, commonly leads to adrenal insufficiency, termed Addison disease. Adrenal insufficiency is also often found in neonates diagnosed prenatally with adrenal calcifications. Therefore, close monitoring of adrenal function is warranted after birth in these cases.
SONOGRAPHY
Adrenal hemorrhage has a variable appearance, depending on the time since hemorrhage occurred. Acutely, the hemorrhage appears as a complex or solid-appearing mass replacing the adrenal gland. The material in the acute hemorrhage may be hyperechoic compared to the adrenal gland or similar in echogenicity. Over time, the hemorrhage organizes and becomes more cystic and hypoechoic, appearing as a cystic mass with internal echoes within the adrenal gland (Figure 15.1.1). Eventually, usually in the postnatal period, the hemorrhage is resorbed completely or decreases in size and becomes calcified.
FIGURE 15.1.1 Adrenal hemorrhage in a fetus with renal vein thrombosis. A: Axial image of upper abdomen showing complex cystic mass (arrows) with internal echoes, located above the kidney. B: Sagittal color Doppler image showing the cystic mass (arrows) superior to echogenic kidney (arrowheads). The kidney is echogenic because the renal vein is thrombosed. C: Video clip through upper abdomen showing cystic mass posterior to the stomach and superior to the left kidney, representing adrenal hemorrhage.


Adrenal calcification appears as a linear echogenic area in the fetal adrenal gland (Figure 15.1.2). It is often bilateral.
2 Hyperplasia
DESCRIPTION AND CLINICAL FEATURES
Adrenal production of corticosteroids may be impaired as a result of a number of genetic conditions. When this occurs, the adrenal glands become enlarged, a condition called congenital adrenal hyperplasia. In some cases, affected female fetuses will have ambiguous genitalia because of altered androgen production. Males with congenital adrenal hyperplasia may have no signs of the condition at birth but will develop symptoms, such as dehydration and poor weight gain, during the first few weeks of life.
SONOGRAPHY
Congenital adrenal hyperplasia is characterized by enlargement of the adrenal glands (Figure 15.2.1). If the fetus is female, ambiguous genitalia may be evident (Figures 15.2.1 and 15.2.2).

3 Masses and Cysts
DESCRIPTION AND CLINICAL FEATURES
Neuroblastoma is the most common adrenal tumor encountered in the fetus. It is a malignant neoplasm and typically grows as pregnancy progresses. Despite this, with postnatal treatment, the prognosis for the child is excellent. Adrenal cysts may be seen rarely and are thought to result from prior hemorrhage, although benign incidental adrenal cysts are occasionally found. Unless the lesion is large and causing symptoms, no intervention is required for these lesions after birth.
SONOGRAPHY
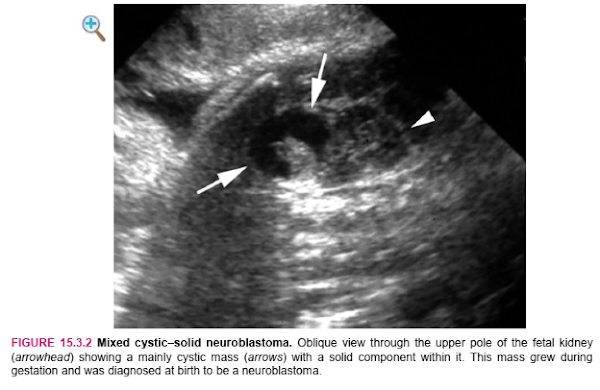
An adrenal neuroblastoma appears as a heterogeneous mass (Figure 15.3.1) in the adrenal gland, sometimes with cystic areas (Figure 15.3.2). They may grow during gestation (Figure 15.3.3) and evidence of rapid growth may prompt delivery.

 |
| FIGURE 15.3.3 Neuroblastoma. A: Transverse image of upper abdomen showing small echogenic mass (arrow) arising from the adrenal gland (arrowhead). B Coronal and (C) sagittal views of the adrenal mass (calipers). This mass grew over the course of the next 2 weeks and was proven to be a neuroblastoma at birth shortly thereafter. |
An adrenal cyst is a well-defined, anechoic lesion in the adrenal gland (Figure 15.3.5).


Nhận xét
Đăng nhận xét