Chapter 19. Placenta
(Atlas of Ultrasound in Obstetrics and Gynecology)
1. Placenta Previa
DESCRIPTION AND CLINICAL FEATURES
Placenta previa refers to a placenta extending to or covering the internal cervical os. When there is a placenta previa at the time of delivery, a vaginal delivery would put the mother and fetus at risk of life-threatening bleeding, and hence, cesarean delivery is indicated.
A variety of terms have been used to classify subtypes of placenta previa, including:
(i) complete previa: one that covers the internal os entirely;
(ii) marginal previa: one that extends to the edge of, but does not cover, the internal os;
(iii) partial previa: one that partially covers the internal os (which can only occur if the internal os is dilated).
The terminology, however, has been used inconsistently at times, with some authors using “partial previa” as synonymous with “marginal previa.” An updated approach to terminology has been recommended by a multisociety workshop that took place in 2012. “Placenta previa” refers to a placenta that covers the internal cervical os, and “low-lying placenta” refers to a placenta that extends to within 2 cm of the internal os. A low-lying placenta in the second or early third trimester frequently
resolves by the mid-to-late third trimester.
Nhau tiền đạo là bánh nhau có vị trí kéo dài đến hoặc bao phủ bên qua cổ tử cung. Khi có nhau tiền đạo tại thời điểm sinh nở, việc sinh ngả âm đạo sẽ khiến mẹ và thai nhi có nguy cơ chảy máu, đe dọa tính mạng và do đó, sinh mổ được chỉ định. Nhiều thuật ngữ đã được sử dụng để phân loại nhau thai tiền đạo, bao gồm:
(i) Nhau tiền đạo toàn phần: một phần bao gồm toàn bộ hệ điều hành nội bộ;
(ii) Nhau bám mép: một phần mở rộng đến cạnh, nhưng không bao phủ, hệ điều hành bên trong;
(iii) Nhau tiền đạo bán phần: một phần che phủ một phần hệ điều hành bên trong (chỉ có thể xảy ra nếu hệ điều hành bên trong bị giãn ra).
Tuy nhiên, những thuật ngữ này đôi khi được sử dụng không nhất quán, với một số tác giả sử dụng “nhau tiền đạo bán phần” đồng nghĩa với “nhau bám mép”. Cập nhật về thuật ngữ đã được khuyến nghị bởi một hội thảo đa khoa diễn ra vào năm 2012. “Nhau tiền đạo” dùng để chỉ nhau thai bao phủ bên trong cổ tử cung và “nhau bám thấp” dùng để chỉ nhau thai kéo dài trong vòng 2 cm của hệ điều hành nội bộ. Nhau bám thấp trong thai quý II hoặc quý III thường xuyên sẽ giải quyết vào 3 tháng giữa đến cuối thai kỳ.
SONOGRAPHY
Placenta previa can be diagnosed by transabdominal or transvaginal sonography. With either of these scanning techniques, a complete previa should be diagnosed when the placenta covers the internal cervical os (Figure 19.1.1), and a low-lying placenta should be diagnosed if the placenta extends to within 2 cm of the os (Figure 19.1.2). Transabdominal sonography is the primary approach to diagnosing placenta previa and should be performed with the bladder partially full. An empty bladder can make visualization of the relevant area difficult, and an overly full bladder can simulate a previa (pseudo-previa) by causing apposition of the anterior and posterior walls of the lower uterine segment. If the lower segment is obscured by the presenting fetal part, manual elevation of the fetus by abdominal palpation is often helpful (Figure 19.1.3). If the presenting part cannot be elevated, transvaginal scanning (Figure 19.1.4) can then be used to assess for previa.
Another pitfall in the diagnosis of placenta previa is when a lower uterine segment contraction is present, distorting the placenta and myometrium to make it appear as though the placenta covers the cervix. In this situation, waiting 10–20 minutes to allow the contraction to resolve will permit the correct diagnosis of previa or no previa (Figure 19.1.5).
Nhau tiền đạo có thể được chẩn đoán bằng siêu âm qua bụng hoặc qua âm đạo. Với một trong hai kỹ thuật này, nên chẩn đoán nhau tiền đạo toàn phần khi nhau thai che phủ mặt trong cổ tử cung (Hình 19.1.1) và nhau bám thấp nên được chẩn đoán nếu nhau thai kéo dài trong vòng 2 cm so với mặt sau (Hình 19.1.1). 19.1.2). Siêu âm bụng là phương pháp chính để chẩn đoán nhau tiền đạo và nên được thực hiện khi bàng quang đầy một phần. Bàng quang trống có thể làm cho việc hình dung khu vực liên quan trở nên khó khăn và bàng quang quá đầy có thể mô phỏng một túi tiền (pseudo-previa) bằng cách gây ra sự sắp xếp của các thành trước và thành sau của đoạn dưới tử cung. Nếu đoạn dưới bị che khuất bởi phần thai hiện diện, thì việc nâng thai bằng tay bằng cách sờ nắn bụng thường hữu ích (Hình 19.1.3). Nếu không thể nâng phần trình bày lên, sau đó có thể sử dụng phương pháp quét qua âm đạo (Hình 19.1.4) để đánh giá phần trước.
Một cạm bẫy khác trong chẩn đoán nhau tiền đạo là khi xuất hiện sự co thắt đoạn dưới tử cung, làm biến dạng nhau thai và cơ tử cung để làm cho nó có vẻ như nhau thai che phủ cổ tử cung. Trong tình huống này, chờ 10–20 phút để cơn co giải quyết sẽ cho phép chẩn đoán chính xác là có tiền đạo hay không (Hình 19.1.5).


transabdominally (A) and transvaginally (B) demonstrate the placenta (PL) with its edge extending to within 2 cm of the internal cervical os (calipers)



2. Nhau bong non
DESCRIPTION AND CLINICAL FEATURES
Placental abruption refers to separation of part or all of the placenta from the uterine wall prior to delivery. The mother often presents clinically with pain and bleeding but may be asymptomatic. Abruption can lead to fetal morbidity or death from hypoxia or exsanguination, and hence, rapid and accurate diagnosis of abruption can be critical to pregnancy management.
Nhau bong non đề cập đến việc tách một phần hoặc toàn bộ nhau thai khỏi thành tử cung trước khi sinh. Người mẹ thường có biểu hiện lâm sàng là đau và chảy máu nhưng có thể không có triệu chứng. Nhau bong non có thể dẫn đến khiếm khuyết hoặc tử vong của thai nhi do thiếu oxy hoặc kiệt sức, và do đó, chẩn đoán nhanh chóng và chính xác nhau bong non có thể rất quan trọng đối với việc quản lý thai nghén.
SONOGRAPHY
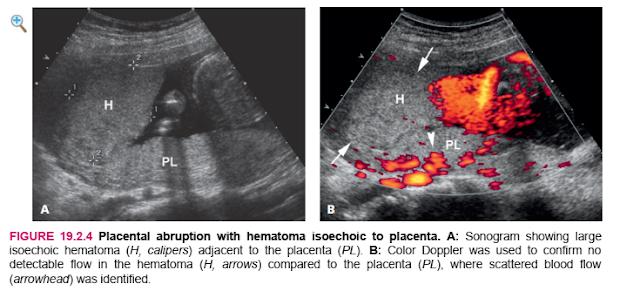
Ultrasound does not detect the placental separation itself but rather can identify a hematoma that might be present with the abruption. The hematoma may be beneath the chorionic membrane (Figure 19.2.1) separate from the placenta, or retroplacental (Figure 19.2.2). Less frequently, it is preplacental (Figure 19.2.3). Hematomas vary in appearance, in that they may appear solid or complex and the solid component may be hypo- or hyperechoic relative to the placenta. If the hematoma is isoechoic to the placenta, color Doppler may aid in its detection (Figure 19.2.4) because the hematoma should be avascular while the placenta is vascular.
Siêu âm không phát hiện được sự tách rời nhau thai khỏi thành tử cung mà có thể xác định được khối máu tụ có thể xuất hiện khi bong nhau. Tụ máu có thể nằm dưới màng đệm (Hình 19.2.1) tách khỏi nhau thai, hoặc trong bánh nhau (Hình 19.2.2). Ít phổ biến hơn, có thể tụ máu trước nhau (Hình 19.2.3). Các khối máu tụ có nhiều dạng khác nhau, trong đó chúng có thể rắn hoặc phức tạp và phần rắn có thể giảm âm hoặc tăng âm so với nhau. Nếu khối máu tụ đồng cản âm với nhau, Doppler màu có thể hỗ trợ việc phát hiện ra nó (Hình 19.2.4) vì khối máu tụ nên vô mạch trong khi nhau thai có mạch máu.

 |
| FIGURE 19.2.2 Placental abruption with retroplacental hematoma. Image of placenta (PL) showing hypoechoic hematoma (H, arrowheads) between the placenta and the uterine wall. |

It is important to note that ultrasound may be normal in a patient with an abruption when there is separation without a hematoma. Thus, identification of a retroplacental or submembranous hematoma is diagnostic of abruption, but a normal sonogram does not rule out abruption.
Điều quan trọng cần lưu ý là siêu âm có thể bình thường ở bệnh nhân vỡ ối khi có sự tách rời mà không có khối máu tụ. Do đó, việc xác định tụ máu dưới màng cứng hoặc dưới màng cứng là chẩn đoán đứt đoạn, nhưng siêu âm thông thường không loại trừ được đứt đoạn.
DESCRIPTION AND CLINICAL FEATURES
The placenta does not normally come into direct contact with the myometrium because these two structures are separated by the decidualized endometrium. If the placenta implants on an area of scarred endometrium, it can attach directly to, or even invade, the myometrium. This abnormal relationship between the placenta and myometrium, which results in difficulty separating the placenta from the uterus at delivery, has been divided into three types:
Accreta: abnormally firm attachment of the placenta to the myometrium
Increta: invasion of chorionic villi into the myometrium
Percreta: penetration of villi through the myometrium, to or through the serosa of the uterus
Nhau thai thường không tiếp xúc trực tiếp với nội mạc tử cung vì hai cấu trúc này bị ngăn cách bởi lớp nội mạc tử cung đã rụng. Nếu nhau thai làm tổ trên một vùng nội mạc tử cung có sẹo, nó có thể bám trực tiếp vào hoặc thậm chí xâm lấn vào nội mạc tử cung. Mối quan hệ bất thường này giữa nhau thai và cơ tử cung, dẫn đến khó tách nhau thai khỏi tử cung khi sinh, đã được chia thành ba loại:
Accreta: sự gắn chặt bất thường của nhau thai vào cơ tử cung
Increta: sự xâm nhập của nhung mao màng đệm vào cơ tử cung
Percreta: sự xâm nhập của nhung mao qua cơ tử cung, đến hoặc qua thanh mạc của tử cung
Placenta accreta, increta, and percreta generally occur when the placenta implants on an area of scarred endometrium, most frequently at the site of a previous cesarean section. A woman who has had one cesarean delivery and whose current pregnancy has a placenta that overlies the cesarean section scar (e.g., a placenta previa or low-lying anterior placenta) is at fairly high risk (approximately 25%) of accreta. The risk of accreta is even higher if she has had two or more cesarean deliveries.
Nhau tích tụ, tăng dần và nhau thai thường xảy ra khi nhau thai làm tổ trên một vùng nội mạc tử cung có sẹo, thường xuyên nhất là tại vị trí của ca mổ lấy thai trước đó. Một phụ nữ đã từng sinh mổ một lần và thai kỳ hiện tại có nhau thai che lấp vết sẹo mổ lấy thai (ví dụ, nhau tiền đạo hoặc nhau tiền đạo nằm thấp) có nguy cơ bị sót nhau khá cao (khoảng 25%). Nguy cơ sót nhau thậm chí còn cao hơn nếu cô ấy đã từng sinh mổ hai lần trở lên.
Placenta accreta, increta, or percreta can lead to a number of serious complications. Difficulty removing the placenta and heavy bleeding at delivery may necessitate hysterectomy. Uterine rupture may result if the placenta is an increta or percreta. Extensive hemorrhage into the bladder or into the peritoneal cavity may occur from placenta percreta.
Placenta accreta, increta, hoặc percreta có thể dẫn đến một số biến chứng nghiêm trọng. Khó loại bỏ nhau thai và chảy máu nhiều khi sinh có thể cần phải cắt bỏ tử cung. Vỡ tử cung có thể xảy ra nếu nhau thai là rau thai hoặc rau câu. Xuất huyết lan rộng vào bàng quang hoặc vào khoang phúc mạc có thể xảy ra do nhau thai.
SONOGRAPHY
The myometrium overlying the placenta normally appears as a hypoechoic band of tissue. With placenta accreta, increta, or percreta, there is a region of marked thinning (Figure 19.3.1) or absence (Figures 19.3.2 to 19.3.4) of this hypoechoic band, sometimes called the “clear zone.” Another common sonographic finding with accreta, increta, or percreta is the presence of large irregular vascular spaces in the placenta, called “lacunae” (Figures 19.3.2 to 19.3.4). Other findings may include exophytic extension or a mass of placental tissue beyond the uterine serosa, blood vessels bridging the uterine–
placental margin or hypervascularity beneath the placenta, and bulging of the uterine contour beneath the placenta.
Cơ tử cung bao phủ nhau thai thường xuất hiện như một dải mô giảm âm. Với lớp đệm nhau thai, increta, hoặc percreta, có một vùng mỏng đi rõ rệt (Hình 19.3.1) hoặc vắng mặt (Hình 19.3.2 đến 19.3.4) của dải giảm âm này, đôi khi được gọi là “vùng trong”. Một phát hiện siêu âm phổ biến khác với accreta, increta, hoặc percreta là sự hiện diện của các khoảng mạch lớn không đều trong nhau thai, được gọi là “lacunae” (Hình 19.3.2 đến 19.3.4). Các phát hiện khác có thể bao gồm sự giãn nở ngoại tiết hoặc một khối mô nhau thai nằm ngoài lớp thanh mạc tử cung, các mạch máu bắc cầu rìa tử cung - nhau thai hoặc sự tăng tuần hoàn bên dưới nhau thai, và sự phồng lên của đường viền tử cung bên dưới nhau thai.




DESCRIPTION AND CLINICAL FEATURES
Chorioangiomas are benign tumors of the placenta. They arise from chorionic tissue and are generally highly vascular. Large chorioangiomas can cause a number of problems, including fetal growth restriction and hydrops. The latter probably occurs as a result of high-output heart failure from vascular shunting through the tumor. Most chorioangiomas, however, cause no pregnancy complications and are incidental findings on sonography or at birth.
SONOGRAPHY
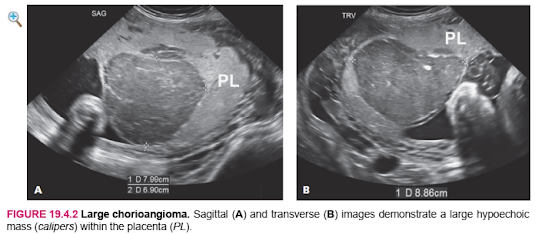
On ultrasound, a chorioangioma appears as a solid hypoechoic mass within the placenta (Figures 19.4.1 and 19.4.2) or projecting from the placenta (Figure 19.4.3). Color Doppler often shows blood flow within the lesion (Figures 19.4.1 and 19.4.3). Chorioangiomas may be difficult to diagnose in the latter part of pregnancy, when the placenta often becomes heterogeneous or may develop infarcts. A focal placental lesion that is distinct in echotexture from the surrounding placenta can be diagnosed as a probable chorioangioma.

When a chorioangioma is diagnosed, the fetus should be scanned to look for evidence of high-output heart failure. An early finding of this is distention of the umbilical vein (Figure 19.4.3) or right atrium. More advanced findings include fetal hydrops, with abnormal fluid collections (pleural or pericardial effusion, ascites, or subcutaneous edema).

Nhận xét
Đăng nhận xét