Chapter 32. Ectopic Pregnancy
(Atlas of Ultrasound in Ob and Gyn)
1. Tubal Ectopic Pregnancy
DESCRIPTION AND CLINICAL FEATURES
Approximately 2% of all pregnancies are ectopic (i.e., implanted at a site other than within the uterine cavity). More than 95% of ectopic pregnancies are located in the fallopian tubes, with most in the isthmic or ampullary portion.
Women whose tubes are scarred or whose pregnancies were achieved by assisted reproductive techniques (e.g., in vitro fertilization) are at elevated risk of ectopic pregnancy. Because the incidence of pelvic inflammatory disease, which can result in tubal scarring, and the use of assisted reproductive techniques have increased over the past two to three decades, ectopic pregnancy has become more frequent than in the past.
Ectopic pregnancy typically presents clinically with pelvic pain and vaginal bleeding. Internal bleeding may occur and may, rarely, be severe enough to cause hypovolemic shock or death, especially if the diagnosis is delayed.
Khoảng 2% các trường hợp mang thai là ngoài tử cung (tức là phôi được cấy tại một vị trí không phải trong khoang tử cung). Hơn 95% thai ngoài tử cung nằm trong ống dẫn trứng, với hầu hết ở phần eo hoặc ống dẫn trứng.
Những phụ nữ có vòi trứng bị sẹo hoặc mang thai bằng kỹ thuật hỗ trợ sinh sản (ví dụ, thụ tinh trong ống nghiệm) có nguy cơ mang thai ngoài tử cung cao hơn. Do tỷ lệ mắc bệnh viêm vùng chậu, có thể dẫn đến sẹo ống dẫn trứng và việc sử dụng các kỹ thuật hỗ trợ sinh sản đã tăng lên trong 2-3 thập kỷ qua, nên việc mang thai ngoài tử cung đã trở nên thường xuyên hơn so với trước đây.
Thai ngoài tử cung thường biểu hiện lâm sàng với đau vùng chậu và chảy máu âm đạo. Chảy máu trong có thể xảy ra và hiếm khi nghiêm trọng đến mức gây sốc giảm thể tích hoặc tử vong, đặc biệt nếu chẩn đoán muộn.
SONOGRAPHY
Ultrasound is the primary diagnostic modality for ectopic pregnancy. When a woman of childbearing age presents with pelvic pain or bleeding and has a positive pregnancy test (sometimes termed a “rule-out-ectopic” patient), ultrasound should be performed emergently and its interpretation should take into account the clinical presentation. In particular, the most likely cause of a complex adnexal mass in a “rule-out-ectopic” patient is ectopic pregnancy, whereas this diagnosis is highly unlikely in a woman with the same sonographic finding but a negative pregnancy test.
Siêu âm là phương thức chẩn đoán chính cho thai ngoài tử cung. Khi phụ nữ trong độ tuổi sinh đẻ có biểu hiện đau vùng chậu hoặc chảy máu và có kết quả thử thai dương tính (đôi khi được gọi là bệnh nhân “chửa ngoài tử cung”), siêu âm nên được thực hiện cấp cứu và việc giải thích cần tính đến biểu hiện lâm sàng. Đặc biệt, nguyên nhân có khả năng cao nhất gây ra một khối phức tạp ở phần phụ ở bệnh nhân “chửa ngoài tử cung” là mang thai ngoài tử cung, trong khi chẩn đoán này rất khó xảy ra ở một phụ nữ có cùng kết quả siêu âm nhưng kết quả thử thai âm tính.
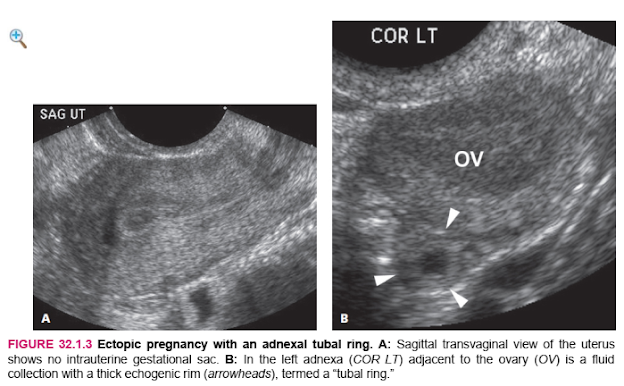
The sonographic finding that is definitive for ectopic pregnancy is visualization of a fluid-filled sac that lies outside the uterine cavity and contains either an embryo with cardiac activity (Figure 32.1.1) or a yolk sac (Figure 32.1.2). A more common, although less definitive, ultrasound finding in a woman with ectopic pregnancy is a complex extraovarian adnexal mass. In some cases, the mass is a fluid collection surrounded by a thick echogenic outer rim, termed a “tubal ring” (Figure 32.1.3), whereas in other cases, the mass has a solid or mixed solid and cystic appearance (Figure 32.1.4). There is sometimes a large amount of free intraperitoneal fluid and/or clotted blood in the pelvis (Figure 32.1.5).
Phát hiện siêu âm xác định mang thai ngoài tử cung là hình dung một túi chứa đầy chất lỏng nằm bên ngoài khoang tử cung và chứa một phôi thai có hoạt động tim (Hình 32.1.1) hoặc một túi noãn hoàng (Hình 32.1.2). Một phát hiện siêu âm phổ biến hơn, mặc dù ít chắc chắn hơn ở một phụ nữ mang thai ngoài tử cung là một khối phụ phức tạp ngoài buồng trứng. Trong một số trường hợp, khối này là một tập hợp chất lỏng được bao quanh bởi một vành ngoài dày có phản âm, được gọi là “vòng ống dẫn trứng” (Hình 32.1.3), trong khi trong các trường hợp khác, khối có dạng rắn hoặc hỗn hợp rắn và dạng nang (Hình 32.1 .4). Đôi khi có một lượng lớn dịch màng bụng tự do và / hoặc máu đông trong khung chậu (Hình 32.1.5).
The adnexal mass representing ectopic pregnancy often has high-volume, low-impedance blood flow around it when interrogated by color or spectral Doppler (Figure 32.1.6). Doppler, however, does not usually help substantially with the diagnosis of ectopic pregnancy because sonographic demonstration of an extraovarian mass and no intrauterine gestational sac in a “rule-out-ectopic” patient indicates a high likelihood (>90%) of ectopic pregnancy, regardless of the Doppler findings.
Khối phần phụ điển hình cho chửa ngoài tử cung thường có lưu lượng máu lớn, trở kháng thấp xung quanh khi được phổ Doppler màu hoặc quang phổ (Hình 32.1.6). Tuy nhiên, Doppler thường không giúp ích đáng kể trong việc chẩn đoán chửa ngoài tử cung vì siêu âm cho thấy một khối ngoài buồng trứng và không có túi thai trong tử cung ở bệnh nhân “chửa ngoài tử cung” cho thấy khả năng cao (> 90%) mang thai ngoài tử cung, bất kể phát hiện Doppler.






2. Interstitial Ectopic Pregnancy
DESCRIPTION AND CLINICAL FEATURES
Interstitial (sometimes termed “cornual”) ectopic pregnancy is one that implants in the interstitial portion of the fallopian tube, the part of the tube that traverses the superolateral aspect of the uterus (the “cornu,” or “horn” of the uterus). This is an uncommon form of ectopic pregnancy but, like other ectopic pregnancies, occurs more frequently in pregnancies achieved via assisted reproductive techniques than those achieved naturally.
A gestational sac implanted in this location can grow for a period of time, but the myometrium around the interstitial portion of the fallopian tube has a far more limited ability to expand than does the body of the uterus. Continued growth of the gestational sac will lead to rupture and potentially life threatening internal bleeding. Fortunately, pain usually occurs earlier than rupture, so prompt diagnosis when the patient presents with symptoms can save the patient’s life or spare her from a hysterectomy. Ultrasound-guided ablation is one of the treatment options.
Thai ngoài tử cung kẽ (đôi khi được gọi là “bắp”) là một thai làm tổ ở phần kẽ của ống dẫn trứng, một phần của ống đi qua mặt bên của tử cung (“bắp” hoặc “sừng” của tử cung) . Đây là một dạng chửa ngoài tử cung không phổ biến nhưng cũng giống như các trường hợp chửa ngoài tử cung khác, xảy ra ở những trường hợp mang thai thông qua kỹ thuật hỗ trợ sinh sản thường xuyên hơn những trường hợp mang thai tự nhiên.
Túi thai được cấy vào vị trí này có thể phát triển trong một khoảng thời gian, nhưng cơ tử cung xung quanh phần kẽ của ống dẫn trứng có khả năng giãn nở hạn chế hơn nhiều so với thân tử cung. Túi thai tiếp tục phát triển sẽ dẫn đến vỡ và chảy máu trong có thể đe dọa tính mạng. May mắn thay, cơn đau thường xảy ra sớm hơn so với vỡ tử cung, do đó, chẩn đoán kịp thời khi bệnh nhân có các triệu chứng có thể cứu sống bệnh nhân hoặc cứu sống bệnh nhân khỏi phẫu thuật cắt bỏ tử cung. Cắt đốt có hướng dẫn bằng siêu âm là một trong những lựa chọn điều trị.
SONOGRAPHY
On ultrasound, interstitial ectopic pregnancy appears as a gestational sac located in the superolateral portion of the uterus, bulging the external uterine contour, with little or no myometrium seen around the lateral or superior aspect of the gestational sac (Figures 32.2.1 and 32.2.2). A high volume of blood flow may be seen around the sac on color Doppler (Figure 32.2.2).
Distinguishing between interstitial ectopic pregnancy and an eccentrically located intrauterine gestation (e.g., a gestational sac in one horn of a bicornuate uterus) can present a diagnostic dilemma. Because the management of these two entities is markedly different—interstitial ectopic pregnancy requires emergent treatment and an eccentrically placed intrauterine gestational sac requires no treatment—it is extremely important to be accurate in distinguishing between them. While the conventional sonographic features described above are generally sufficient to establish the diagnosis, 3D ultrasound with a true coronal view of the uterus can be useful by providing a clear depiction of the uterine cavity an gestational sac (Figures 32.2.1 and 32.2.2).
Trên siêu âm, chửa ngoài tử cung kẽ xuất hiện như một túi thai nằm ở phần bên ngoài của tử cung, phình ra ở đường viền ngoài tử cung, ít hoặc không thấy cơ tử cung xung quanh mặt bên hoặc mặt trên của túi thai (Hình 32.2.1 và 32.2. 2). Có thể thấy một lượng máu chảy nhiều quanh túi trên Doppler màu (Hình 32.2.2).
Việc phân biệt giữa thai ngoài tử cung kẽ và thai trong tử cung nằm lệch tâm (ví dụ, một túi thai trong một sừng của tử cung hai bên) có thể đưa ra một tình huống khó chẩn đoán. Vì cách xử trí của hai thực thể này khác nhau rõ rệt - chửa ngoài tử cung kẽ cần điều trị khẩn cấp và túi thai đặt lệch tâm không cần điều trị - điều cực kỳ quan trọng là phải phân biệt chính xác giữa chúng. Mặc dù các đặc điểm siêu âm thông thường được mô tả ở trên nói chung là đủ để xác định chẩn đoán, siêu âm 3D với hình ảnh tử cung thực sự có thể hữu ích bằng cách cung cấp mô tả rõ ràng về khoang tử cung và túi thai (Hình 32.2.1 và 32.2.2) .


3. Cervical Ectopic Pregnancy
DESCRIPTION AND CLINICAL FEATURES
Cervical ectopic pregnancy is one that implants in the cervix. This form of ectopic pregnancy is very rare in naturally conceived pregnancies. Although it is found more frequently in pregnancies achieved via assisted reproductive techniques, it is still an extremely uncommon occurrence. A gestational sac implanted in the cervix typically causes symptoms of pelvic pain and vaginal bleeding before the mid first trimester. The bleeding can be heavy enough to be lifethreatening to the mother if not treated promptly.Before the availability of ultrasound, the diagnosis of cervical ectopic pregnancy was often made from the surgical specimen after a woman underwent a hysterectomy for uncontrollable vaginal bleeding. With ultrasound, the diagnosis can be made earlier, thus permitting treatments that leave the uterus intact.
Thai ngoài tử cung là một thai làm tổ trong cổ tử cung. Dạng chửa ngoài tử cung này rất hiếm gặp ở những trường hợp mang thai tự nhiên. Mặc dù nó được tìm thấy thường xuyên hơn trong các trường hợp mang thai thông qua các kỹ thuật hỗ trợ sinh sản, nhưng nó vẫn là một trường hợp cực kỳ không phổ biến. Túi thai được cấy vào cổ tử cung thường gây ra các triệu chứng đau vùng chậu và chảy máu âm đạo trước 3 tháng giữa của thai kỳ. Máu chảy ra có thể nặng đến mức nguy hiểm đến tính mạng của người mẹ nếu không được điều trị kịp thời. Với siêu âm, chẩn đoán có thể được thực hiện sớm hơn, do đó cho phép các phương pháp điều trị để lại tử cung nguyên vẹn.
SONOGRAPHY
With cervical ectopic pregnancy, ultrasound demonstrates a gestational sac in the cervix, often containing a yolk sac or embryo (Figures 32.3.1 and 32.3.2). Two diagnostic dilemmas can arise in the sonographic diagnosis of cervical ectopic pregnancy: (1) distinguishing between cervical ectopic pregnancy and a miscarriage in progress and (2) distinguishing between a sac implanted in the cervix and one implanted in the lower uterine segment. The first distinction can usually be made based on the appearance of the intracervical gestational sac. A well-formed, round or oval sac surrounded by a thick echogenic rim is highly suggestive of cervical ectopic pregnancy, particularly if an embryo with cardiac activity is seen within the sac. On the other hand, a gestational sac that began in the uterine body and is in the process of passing through the cervix is typically flattened, has little or no echogenic rim, and is empty or has a dead embryo within it. When there is uncertainty about the correct diagnosis, rescanning a day or two later will generally clarify the matter: an unchanged appearance is indicative of cervical ectopic pregnancy, whereas the disappearance or marked change in appearance of the sac indicates a miscarriage in progress.
Với chửa ngoài tử cung, siêu âm chứng tỏ có túi thai trong cổ tử cung, thường chứa túi noãn hoàng hoặc phôi thai (Hình 32.3.1 và 32.3.2). Hai tình huống khó chẩn đoán có thể nảy sinh trong chẩn đoán siêu âm thai ngoài tử cung: (1) phân biệt giữa chửa ngoài tử cung và sẩy thai đang diễn ra và (2) phân biệt giữa một túi được cấy trong cổ tử cung và một túi được cấy vào đoạn dưới tử cung. Sự phân biệt đầu tiên thường có thể được thực hiện dựa trên sự xuất hiện của túi thai trong cổ tử cung. Một túi hình tròn hoặc bầu dục được hình thành tốt được bao quanh bởi một vành hồi âm dày rất gợi ý mang thai ngoài tử cung, đặc biệt nếu phôi thai có hoạt động tim được nhìn thấy trong túi. Mặt khác, một túi thai bắt đầu trong thân tử cung và đang trong quá trình đi qua cổ tử cung thường bị dẹt, có ít hoặc không có vành hồi âm, và trống rỗng hoặc có phôi thai chết bên trong. Khi không chắc chắn về chẩn đoán chính xác, việc quét lại một hoặc hai ngày sau nói chung sẽ làm rõ vấn đề: hình dạng không thay đổi là dấu hiệu của thai ngoài tử cung, trong khi sự biến mất hoặc thay đổi rõ rệt về hình dạng của túi cho thấy một sẩy thai đang diễn ra.
Distinguishing between cervical and lower segment implantation can usually be made by transvaginal ultrasound based on the distance between the gestational sac and the transducer. With cervical ectopic pregnancy, the sac is generally within 1–2 cm of the transducer
Việc phân biệt giữa làm tổ ở cổ tử cung và đoạn dưới thường có thể được thực hiện bằng siêu âm qua ngã âm đạo dựa trên khoảng cách giữa túi thai và đầu dò. Với chửa ngoài tử cung, túi thường nằm trong vòng 1–2 cm tính từ đầu dò
 |
| FIGURE 32.3.1 Cervical ectopic pregnancy on transvaginal sonography. A: Sagittal transvaginal view of the uterus demonstrates a gestational sac (arrow) with yolk sac (arrowhead). The gestational sac lies within the cervix, not the body of the uterus. B: Close-up view of the embryo (calipers) within the intracervical gestational sac. Embryonic cardiac activity was seen on real-time sonography. C: 3D image demonstrates the gestational sac (long arrow) within the cervix (short arrow), and not in the uterine body. D: Video clip showing embryonic cardiac activity within the cervical ectopic pregnancy.
|

DESCRIPTION AND CLINICAL FEATURES
A pregnancy implanted on the scar from a prior cesarean delivery is a form of abnormally located pregnancy, though not technically an ectopic pregnancy. These pregnancies can lead to two types of adverse events. If the sac extends deeply into the scar, reaching the serosal surface of the uterus during the first trimester, uterine rupture may occur as the gestational sac grows. The rupture can cause internal bleeding that is life-threatening to the mother. Early diagnosis can lead to treatment that saves the life of the mother and preserves the uterus.
The second adverse event that can occur with implantation on the cesarean scar is development of placenta accreta. This complication occurs when the gestational sac grows predominantly within the uterine cavity adjacent to the scar, but the placenta invades the myometrium at the site of the scar.
Thai được cấy vào vết sẹo do mổ lấy thai trước đó là một dạng thai nằm bất thường, mặc dù về mặt kỹ thuật không phải là thai ngoài tử cung. Những lần mang thai này có thể dẫn đến hai loại biến cố bất lợi. Nếu túi mở rộng sâu thành sẹo, chạm đến bề mặt thanh mạc của tử cung trong tam cá nguyệt đầu tiên, có thể xảy ra vỡ tử cung khi túi thai lớn lên. Vết vỡ có thể gây chảy máu trong nguy hiểm đến tính mạng của mẹ. Chẩn đoán sớm có thể dẫn đến điều trị cứu sống người mẹ và bảo tồn tử cung.
Tác dụng phụ thứ hai có thể xảy ra khi cấy vào vết sẹo mổ lấy thai là sự phát triển của nhau thai. Biến chứng này xảy ra khi túi thai phát triển chủ yếu trong khoang tử cung tiếp giáp với sẹo, nhưng nhau thai xâm lấn vào cơ tử cung tại vị trí sẹo.
SONOGRAPHY
In a woman who has undergone prior cesarean delivery, ultrasound diagnosis of a pregnancy implanting deep into a cesarean scar is established when the gestational sac is located in the anterior lower uterine segment and the echogenic wall of the sac extends close to the serosal surface of the uterus (Figure 32.4.1). The gestational sac is often triangular in shape, pointing toward the anterior serosal surface of the uterus (Figure 32.4.1). There may be extensive blood flow around the gestational sac (Figure 32.4.2). If left untreated, sequential scans may demonstrate progressive bulging of the uterine contour (Figure 32.4.3).
Ở một phụ nữ đã từng sinh mổ trước đó, siêu âm chẩn đoán thai làm tổ sâu trong sẹo mổ lấy thai khi túi thai nằm ở đoạn trước dưới tử cung và thành hồi âm của túi kéo dài đến gần bề mặt thanh mạc của tử cung (Hình 32.4.1). Túi thai thường có hình tam giác, hướng về mặt thanh mạc trước của tử cung (Hình 32.4.1). Có thể có máu chảy nhiều quanh túi thai (Hình 32.4.2). Nếu không được điều trị, chụp quét tuần tự có thể cho thấy đường viền tử cung ngày càng phình ra (Hình 32.4.3).

 |
FIGURE 32.4.2 Highly vascular cesarean scar pregnancy implantation. (A) Sagittal and (B) coronal images demonstrate a gestational sac (long arrow) in the lower uterine segment extending to the anterior serosal surface of the uterus (short arrow). An embryo (arrowhead) is seen within the gestational sac and a hematoma (*) is present around the sac. C: Color Doppler demonstrates extensive blood flow around the sac. D: Video clip demonstrates embryonic cardiac activity. HÌNH 32.4.2 Chửa thai có sẹo mổ lấy thai có nhiều mạch máu. (A) Hình ảnh Sagittal và (B) coronal chứng minh một túi thai (mũi tên dài) ở đoạn dưới tử cung kéo dài đến bề mặt thanh mạc trước của tử cung (mũi tên ngắn). Một phôi thai (đầu mũi tên) được nhìn thấy trong túi thai và một khối máu tụ (*) là hiện xung quanh túi. C: Doppler màu cho thấy dòng máu chảy nhiều quanh túi. D: Video clip chứng tỏ hoạt động của tim phôi. |

DESCRIPTION AND CLINICAL FEATURES
Abdominal ectopic pregnancy is an extremely rare form of ectopic pregnancy in which the gestational sac implants in the peritoneal cavity. This type of ectopic pregnancy can occur when the pregnancy implants directly in the abdomen, or it can occur when the pregnancy begins as a tubal ectopic and then reimplants in the abdomen after the fallopian tube ruptures or the gestational sac is expelled through the end of the tube. The maternal mortality rate with abdominal pregnancies is severalfold higher than with other forms of ectopic pregnancy, due to the high incidence of internal hemorrhage. In many abdominal pregnancies, the fetus dies early in gestation. In some cases, however, the fetus can remain alive until the second or even the third trimester, and may rarely lead to a liveborn infant.
Treatment consists of surgical removal of the fetus and placenta, unless the latter cannot be resected safely from the major blood vessels or abdominal organs. If some or all of the placenta is left in place, it may take several months to resorb.
In the early-to-mid first trimester, abdominal pregnancy may be indistinguishable from tubal ectopic pregnancy on ultrasound. In the late first trimester and beyond, demonstration of a live fetus outside the uterus is highly suggestive of abdominal pregnancy, because the fallopian tube cannot contain a pregnancy that large. Because abdominal pregnancy may be contiguous with the fundus of the uterus, it is essential to delineate the margin of the uterus carefully to demonstrate that the gestational sac lies outside the uterus (Figure 32.5.1).
If surgery is performed and the placenta cannot be removed in its entirety, ultrasound plays a useful role in monitoring the patient. In particular, ultrasound can follow the placenta until it resorbs completely, and can assess for complications of the retained placenta, such as abscess or hemorrhage.


 |
FIGURE 32.6.2 Heterotopic pregnancy: interstitial ectopic and intrauterine gestational sacs. A: Transverse transabdominal view of the uterus demonstrates two gestational sacs, one within the uterus (long arrow) and one an interstitial ectopic pregnancy (short arrow). B: Video clip showing cardiac activity in both the intrauterine and interstitial ectopic embryos. HÌNH 32.6.2 Thai dị sản: các túi thai ngoài tử cung và trong tử cung có kẽ. A: Ngang nhìn qua bụng của tử cung cho thấy hai túi thai, một trong tử cung (mũi tên dài) và một chửa ngoài tử cung ở kẽ (mũi tên ngắn). B: Video clip cho thấy hoạt động của tim trong cả tử cung và phôi ngoài tử cung kẽ. |
Nhận xét
Đăng nhận xét