(Choice B) Generally, zidovudine therapy alone is administered to the infant However, for mothers who did not receive antenatal antiretroviral therapy, the addition of nevirapine therapy to the infant's regimen can reduce the risk of maternal-to-child HIV transmission.
(Choice C) Post-exposure prophylaxis with viral-specific immunoglobulin can be helpful in infections such as hepatitis Band rabies. Unfortunately, HIV immunoglobulin therapy is currently unavailable. Pooled immunoglobulin G does not have high titers of the desired HIV antibody to be reliably effective.
(Choice E) Forceps or any procedure that can tear the infant's skin should be avoided due to increased risk of HIV transmission.
Educational objective:
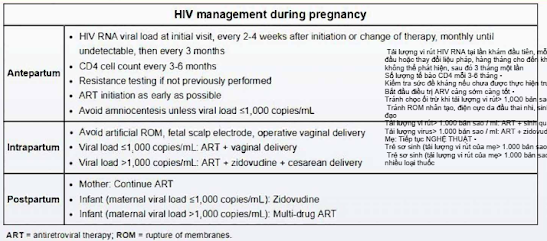
Maternal combination antiretroviral therapy during pregnancy and neonatal zidovudine therapy can reduce perinatal HIV transmission to <1%. If the diagnosis is made late in the pregnancy, intrapartum zidovudine and infant treatment should still be offered.
Can thiệp quan trọng nhất để ngăn ngừa sự lây lan của HIV từ mẹ sang con là sử dụng điều trị ARV phối hợp cho người mẹ trong suốt thai kỳ. Điều trị kháng vi-rút nên được bắt đầu càng sớm càng tốt trong thời kỳ mang thai (ngay cả trong ba tháng đầu), bất kể số lượng CD4 của mẹ hoặc tải lượng vi-rút. Điều trị phối hợp trước sinh là cách tốt nhất để ngăn chặn HIV ở người mẹ và ngăn ngừa lây nhiễm qua nhau thai hoặc chu sinh ở trẻ sơ sinh Những bà mẹ có tải lượng vi rút không phát hiện được khi sinh có nguy cơ truyền nhiễm cho trẻ <1%. Phác đồ 3 thuốc nên bao gồm 2 chất ức chế men sao chép ngược nucleoside (NRTls) cộng với một chất ức chế men sao chép ngược không nucleoside hoặc một chất ức chế protease. Nên sử dụng NRTI có khả năng truyền qua nhau thai tốt (ví dụ như zidovudine, tenofovir). Zidovudine nên được dùng cho trẻ sơ sinh trong 6 tuần.
(Lựa chọn A) Mổ lấy thai có chọn lọc đã được chứng minh là có lợi nếu tải lượng vi rút của người mẹ khi sinh> 1.000 bản sao / ml, vì nó có thể làm giảm 50% sự lây truyền HIV chu sinh. Zidovudine cộng với mổ lấy thai tự chọn làm giảm nguy cơ lây truyền hơn so với can thiệp đơn thuần. Tuy nhiên, liệu pháp kháng vi-rút kết hợp có hiệu quả hơn bất kỳ chiến lược nào trong số các chiến lược này trong việc ngăn ngừa nhiễm HIV sơ sinh.
(Lựa chọn B) Nói chung, chỉ dùng liệu pháp zidovudine cho trẻ sơ sinh Tuy nhiên, đối với những bà mẹ không được điều trị ARV trước sinh, việc bổ sung liệu pháp nevirapine vào phác đồ của trẻ sơ sinh có thể làm giảm nguy cơ lây truyền HIV từ mẹ sang con.
(Lựa chọn C) Dự phòng sau phơi nhiễm bằng globulin miễn dịch đặc hiệu với virus có thể hữu ích trong các bệnh nhiễm trùng như bệnh dại do viêm gan Band. Thật không may, liệu pháp globulin miễn dịch HIV hiện không có sẵn. Globulin miễn dịch gộp chung G không có hiệu giá cao của kháng thể HIV mong muốn để có hiệu quả đáng tin cậy.
(Lựa chọn E) Cần tránh dùng kẹp hoặc bất kỳ thủ thuật nào có thể làm rách da trẻ sơ sinh do tăng nguy cơ lây truyền HIV.
Mục tiêu giáo dục:
Điều trị ARV kết hợp cho bà mẹ trong thời kỳ mang thai và điều trị zidovudine sơ sinh có thể giảm lây truyền HIV chu sinh xuống <1%. Nếu chẩn đoán được thực hiện muộn trong thai kỳ, vẫn nên cung cấp zidovudine trong sinh và điều trị cho trẻ sơ sinh.
Nhận xét
Đăng nhận xét