Chapter 15 Bartholin Duct and Gland Surgery

GENERAL PRINCIPLES
Definition
The physiologic Bartholin gland is a nonpalpable structure 12 mm deep to the vaginal mucosal surface. Two bilateral glands drain into orifices located at 5 and 7 o’clock positions between the hymenal ring and labia minora. The misnomer, Bartholin cyst, is often used to describe the obstructed and dilated, but sterile and nonpainful, Bartholin gland and duct. An encapsulated Bartholin abscess may elicit vulvar pain with sitting or walking. Less frequently, a Bartholin abscess may be associated with fevers or chills. Progression is not always the necessary path to abscess formation.
Differential Diagnosis
■ Bartholin adenocarcinoma or squamous cell carcinoma
■ Folliculitis
■ Leiomyoma
■ Lipoma
■ Vulvar dysplasia/cancer
■ Vaginal dysplasia/cancer
■ Skene’s and Gartner duct cysts
■ Necrotizing fasciitis
■ Perirectal abscess
■ Canal of Nuck cyst
■ Fibroma
■ Epidermal inclusion cyst
Anatomic Considerations
The Bartholin gland, also known as the greater vestibular gland, is located in the superficial compartment of the vulva, near the introitus. The gland comprised of mucinous acini, and the duct is a combination of transitional epithelium, mucinous cells, and squamous epithelium. The orifices are lined with squamous epithelium. Supplying the gland are numerous branches of the inferior pudendal artery. Deep to the gland is a thick network of anastomosing venous channels, known as the vestibular bulb. It is this erectiletissue of the vestibular bulb that contributes to the bloody nature of the Bartholin gland excision. Occasionally, during large gland excisions, other surrounding structures can be appreciated. The ischiorectal fossa is a relatively avascular area that has notorious potential for infection to manifest and spread to surrounding pelvic compartments.
Nonoperative Management
Management may entail observation, sitz baths, antibiotics, silver nitrate ablation, CO2 laser vaporization, epithelialization with Word or Jacobi ring, marsupialization, and excision. None has proven to be superior, but ideal treatment would be fast, safe, performed with local anesthesia in outpatient setting, and with low recurrence and fast healing. Observation is sufficient for the painless Bartholin duct cyst that may even reach several centimeters in size in the otherwise-healthy individual under the age of 40. If the patient has no signs of systemic infection, advise sitz baths alone for the spontaneously draining abscess or pointed abscess that is almost ready to drain. Antibiotic therapy is the first-line treatment for an abscess that is not yet matured for drainage and is the second-line therapy for an abscess that has not clinically improved after drainage. Evaluate the need for antibiotics as adjunctive treatment at the time of drainage. Patients with the following comorbidities and/or sign and symptoms should be treated with antibiotics at the time of drainage: diabetes, immunosuppression, pregnancy, high MRSA risk, recurrent infection, or signs of cellulitis or systemic infection. A broad-spectrum antibiotic that covers Gram-negative and Gram-positive organisms over anaerobes such as amoxicillin clavulanate 875 mg PO q12h for 7 days, or trimethoprim sulfamethoxazole 800/160 PO q12h for 7 days is sufficient. For augmented MRSA and Bacteroides coverage, consider adding clindamycin 300 mg PO four times a day for 7 days. An Israeli study by Kessous et al. confirmed Escherichia coli as the most common organism cultured from 43.7% of Bartholin gland infections. Empiric treatment with amoxicillin clavulanate was associated with recurrence averages between 32 and 50 months.
Historically, Bartholin abscesses were attributed to sexually transmitted infections, but recently, this notion has been disproven by Hoosen, Tanaka, and Kessous. STD testing may be offered at the time of Bartholin abscess presentation but antibiotic choice should not empirically encompass Neisseria gonorrhea or Chlamydia trachomatis.
Characteristics of an abscess, that require prompt operative, rather than nonoperative management, include abscess recurrence, pain and erythema, fever, and fluctuance. Of note, although incision and drainage (I&D) may offer symptomatic relief of an acutely painful abscess, I&D alone, although described in some studies, is generally not recommended because it confers no long-term benefit and increases the risk of recurrence up to 38%. Instead,drainage with the goal of epithelializing an egress tract from the gland is preferred. This may be accomplished with silver nitrate ablation, CO2 laser,
Word catheter or Jacobi ring placement, or marsupialization. The following patients and conditions require biopsy in addition to drainage: women over 40, immune-compromised patients, history of Paget’s disease, history of any gynecologic malignancy, and those with recurrent abscess formation. Complete surgical excision should be performed instead of biopsy in postmenopausal women and when the Bartholin mass is firm and irregular.
Silver Nitrate Ablation
Various silver nitrate techniques have been described, all with the goal of gland destruction. A silver nitrate technique from Turkey was compared to marsupialization and found to have similar recurrence rates (26% and 24%) and time to recurrence (2 and 1.5 months); however, the side effects of the treatments differed. Chemical burn and hematoma formation occurred, compared to discharge from marsupialization.
CO2 Laser
CO2 laser treatment is an outpatient procedure performed under local anesthesia. The laser is used to vaporize, fenestrate, or excise Bartholin lesions with a recurrence rate of 10%. It is less optimal for lesions which are hyperechogenic, multiloculated, and with wall thickness 0.5 to 1.5 mm. Ultrasound, CO2 laser accreditation, and pre- and postprocedure antibiotics are necessary for this technique. Specific social factors significantly associated with likelihood of recurrence were elevated stress, use of synthetic clothing, and use of condoms.
Indwelling Devices: Word Catheter or Jacobi Ring drainage of the obstruction coupled with placement of a Word catheter or Jacobi ring, both of which are placed in the outpatient setting under local anesthesia, have recurrence rates of 4% to 17%.
Biopsy
Any Bartholin gland enlargement in the woman over 40 is considered malignant until proven otherwise by biopsy. In any of these procedures, a biopsy of the superficial gland wall can be excised with sharp scissors and submitted to pathology; however, biopsies must be amply large to be of use.
Marsupialization
Although its role is largely replaced by outpatient Word catheter placement; marsupialization offers guaranteed epithelialization of the Bartholin gland in the setting of recurrent abscess formation and is an option with less morbiditythan Bartholin gland excision. Perform marsupialization after the patient has failed one to two Word catheters or Jacobi ring placements, and when the gland is not acutely inflamed, to avoid risk of infection.
Excision
Bartholin gland excision is quintessentially one of the bloodiest of the small gynecologic procedures. Excision is rarely required for the young patient, as the sequelae often can include dyspareunia from either lack of lubrication due to removal of the mucin-producing cells, or more commonly, from obstruction of any residual duct. In women over 40, where malignancy is of greater concern, gland excision permits a definitive evaluation and is chosen when other methods have failed; however, biopsy is still preferred over excision.
Adenocarcinoma of the Bartholin gland is exceedingly rare, comprising 1% of all vulvar cancers. Nearly 50% of suspected adenocarcinomas of the Bartholin gland are in fact squamous cell carcinomas. If the deeper gland surface is palpated to have a mass, consider excision due to proximity to underlying vestibular bulb. If a mass persists after a normal biopsy result, perform excision. Ulceration and persistent dyspareunia, a solid mass, or a mass in a slightly different location than the usual Bartholin duct could be other indications of Bartholin malignancy that require excision of the entire gland for definitive diagnosis.
IMAGING AND OTHER DIAGNOSTICS
■ Imaging is not routinely utilized for Bartholin pathology. History and physical examination dictate management decisions.
PREOPERATIVE PLANNING
■ Perform a pelvic examination under anesthesia with careful attention to the size, shape, and direction of the Bartholin gland prior to surgical management. Include a rectal examination to evaluate the proximity of the gland to the rectum in cases of excision.
SURGICAL MANAGEMENT
Epithelialization
Creating an intentional fistula, or epithelialization of a Bartholin gland abscess, is superior to simple I&D as the fistula prevents future abscess formation.
Silver Nitrate Ablation
■ This outpatient technique is performed with local anesthesia.
■ The gland is incised, two stay sutures are placed to retract the glandmargins and a 0.5 × 0.5 cm piece of silver nitrate is placed in the cavity. The sutures are then tied to re-approximate the gland.
■ At day 3, the sutures and silver nitrate are removed. Antibiotics are only prescribed in the case of abscess.
CO2 Laser
■ The laser is used to create a 10 to 15 mm circular lesion on the overlying mucosal surface, and after drainage, the gland surface, including all loculations, is vaporized with a depth of destruction of 2 mm, excised, orleft fenestrated.
Word Catheter
■ The Word catheter is a latex-free silicone-based indwelling device.

Figure 15.1. A and B: Inflate the Word catheter with 3 mL of sterile liquid.
■ Cleanse the mucosa overlying the Bartholin gland and vaginal mucosa with antiseptic solution and then retract open.
■ Inject the mucosa near the hymenal ring that is overlying the Bartholin gland with 1 to 2 cc of 1% lidocaine without epinephrine. Depending on the size of the gland, exposure to the mucosa may best be accomplished by applying pressure to reflect the gland out of the vagina.
■ Make a 2 to 3 mm incision with the 11 blade scalpel over the most gravitydependent mucosa ideally inside, but if necessary on or just outside the hymenal ring.
■ Probing inside the gland is not recommended, as this can overly stretch the length of this incision, and then the Word catheter will fall out.
■ Allow the contents of the abscess to drain, then insert the deflated catheter. Inflate the balloon with up to a maximum of 3 mL of sterile liquid, not air.
Use caution so as not to puncture this tiny balloon with either the syringe upon inflation or by over-distention.
■ Remove the syringe and tuck the catheter inside the vagina. The Word catheter should remain in place for 3 to 4 weeks, to ensure the tract becomes epithelialized and ideally prevent future obstruction (Fig. 15.1).
■ If the gland size is too small to accommodate the Word catheter, other indwelling drainage options are available. If office supplies are at hand, the gland can be marsupialized. Otherwise, I&D will have to suffice until further management can be planned.
Jacobi Ring
The Jacobi ring is an alternative to the Word catheter. It is a tubular structure with a threaded suture that is passed into and out of the gland through two separate incisions and then tied into a 360-degree ring. The ring establishes an egress and promotes prolonged fenestration.
■ Construct the ring catheter from 7 cm of an 8-French rubber T tube
threaded with a 20 cm length of 2-0 silk suture.
■ Cleanse the area and inject local anesthetic, then make a 3-mm incision with the 11 blade scalpel on the mucosal surface.
■ Pass a hemostat through the abscess to tunnel and make the indentation for the second incision.
■ Pull one end of the Jacobi ring through the abscess incisions. Tie the twoends together. Use caution not to tie too tightly, as ischemia can occur (Fig. 15.2).
Positioning
■ The patient is placed in the dorsal–lithotomy position with careful attention not to hyperflex or hyperextend the legs and hips. The patient is then prepped and draped in the usual fashion for a vaginal procedure.

Figure 15.2. Steps for Jacobi ring insertion for epithelialization of the Bartholin gland.Procedures and Techniques (Video 15.1)
Biopsy
■ Biopsy is performed by excision of cyst wall at the time of drainage when a small sample of gland wall can be excised with the scalpel. During marsupialization, send the elliptical portion of gland wall to pathology.
Marsupialization
■ Marsupialization is performed under local or general anesthesia. Perform a digital vaginal examination to delineate the borders of the gland.
■ With a 15 blade scalpel, make a generous vertical incision the length of the cyst along the hymenal ring.
■ To incise and drain the gland, make an elliptical incision through the wall of the gland.
■ Evert gland edges and mucosal edges with atraumatic grasping forceps, then suture the wall of the gland to squamous epithelium of the introitus laterally and to vaginal mucosa medially with interrupted horizontal mattress stitches with 3-0 polysorb. Place sutures at least 5 mm from everted glandular wall to epithelial tissue to increase success of marsupialization procedure (Tech Fig. 15.1).
■ Potential consequences are infection and recurrence of cyst if the opening scars shut.

Tech Figure 15.1. The hymenal ring is the preferred location for epithelialization, marsupialization, and the initial incision of gland excision due to optimal tissue healing and cosmesis. Photo courtesy of M. Walters, MD.
Bartholin gland excision
■ Begin the procedure with a digital rectovaginal examination to appreciate theborders of the gland and proximity to the vaginal wall and rectum. The deep base of the gland is supplied by branches of the inferior pudendal artery, a branch of the internal iliac artery. The vestibular bulb drains the gland and is a network of venous channels.
■ Empty the bladder with straight catheterization.
■ Retract the labia laterally with Allis clamps.
■ Inject 1% lidocaine with epinephrine into the mucosa along the hymenal ring, but notably, not into the gland.
■ Over the vaginal mucosal side of the gland, just on or inside the hymenal ring, use a 15 blade scalpel to create a superficial long vaginal mucosa incision, with careful attention to avoid simultaneously incising the gland (Tech Fig. 15.2). The mucosa is the preferred site because it heals faster and is less painful than the epidermal vulvar skin. Retract the mucosa and expose the gland. Infection may fuse the borders between the gland and mucosa.
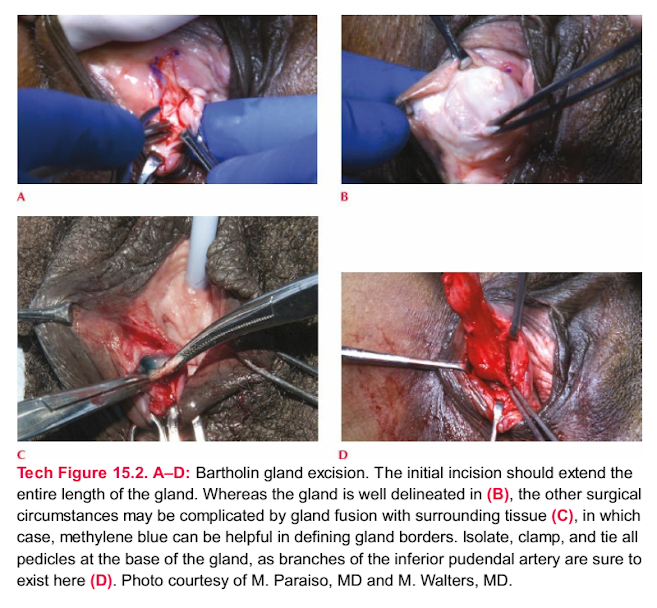
Tech Figure 15.2. A–D: Bartholin gland excision. The initial incision should extend the entire length of the gland. Whereas the gland is well delineated in (B), the other surgical circumstances may be complicated by gland fusion with surrounding tissue (C), in which case, methylene blue can be helpful in defining gland borders. Isolate, clamp, and tie all pedicles at the base of the gland, as branches of the inferior pudendal artery are sure to exist here (D). Photo courtesy of M. Paraiso, MD and M. Walters, MD.

Tech Figure 15.3. A–D: Closure after gland excision occurs in multiple layers. Reapproximating the dead space is an initial measure to prevent bleeding from the venous network comprising the vestibular bulb. Photo courtesy of M. Walters, MD.
■ Delineate the plane between mucosa and gland with traction and countertraction and Metzenbaum scissors. Dilute methylene blue can be injected for purposes of demarcating the gland during excision (Tech Fig. 15.2). Grasp and retract the gland wall with the Allis clamp to facilitate dissection and visualization of blood supply.
■ Bleeding must be anticipated and hemostasis must be achieved with each step. Clamp any vascular pedicles with a fine-tipped clamp, cut, and suture ligate with 3-0 absorbable suture (Tech Fig. 15.2).
■ Entire removal of the gland is crucial, as residual glandular tissue may cause recurrence of cyst or abscess and may be responsible for chronic pain. Evaluate for multiloculated remaining abscess. If the margins of the gland are fused to surrounding tissue because of infection, open the gland, place a finger in the gland, and proceed with dissection from this angle. A lacrimal duct probe can be inserted into the gland to mark the gland.
■ Once the entire gland is removed, hemostasis must be achieved, namely with suture ligation, but also with electrosurgery, hemostatic agents, and, ultimately, obliteration of the dead space with a multilayered closure. Electrocautery alone is insufficient. Once a bleeding vessel retracts and bleeding continues, dissect further and tie the vessel. The entire cavity must be closed with interrupted 3-0 absorbable suture, in multiple layers (Tech Fig. 15.3). Use caution to avoidplacing a stitch through the labia. Interrupted stitches are preferred over running stitches as running stitches may cause abnormal scarring and pain.
■ If necessary, in the circumstance of infected gland with purulent drainage, a drain may be stitched into the wound closure with 5-0 interrupted absorbable suture to ensure drainage.
■ Close the vaginal mucosa with interrupted 3-0 delayed absorbable suture around the drain. Perform a rectal examination at the conclusion of the case to ensure the rectum and vaginal wall are free of suture. Remove the drain on postoperative day 3 or 4.
PEARLS AND PITFALLS
The Word catheter is likely to fall out if the balloon is perforated by overfilling, if the incision is made too wide, or if the depth of the deflated gland is too shallow. \
Cook medical manufacturing instructions indicate the maximum volume of the bulb is 3 mL.
The preferred location of Bartholin surgeries is on or inside the hymenal ring for the purposes of tissue healing, cosmesis, and pain.
Surgeries performed outside the hymenal ring can result in distorted anatomy, which can contribute to chronic pain.
Keeping the abscess intact during excision allows for easy delineation of borders and gland removal.
If the abscess is entered, keep a lacrimal duct probe in the open gland. Apply traction to the walls. Use fine clamps and fine scissors to delineate borders for the remainder of the excision.
Achieve hemostasis with each step of excision with the clamp, cut, and tie suture ligation technique.
Unidentified sources of bleeding can result in hematoma formation and postoperative complications.
Evaluate carefully for multi-loculated abscess and remove entire abscess upon excision.
Residual gland after excision will have incomplete results with abscess reformation and chronic pain.
POSTOPERATIVE CARE
■ Postoperative perineal lavage bottles are recommended and wound packing is not necessary. Drainage is to be expected. The area should be kept clean and dry and can be accomplished with the cool setting of the hair dryer. Pelvic rest is recommended for 4 weeks.
COMPLICATIONS
■ Vulvar hematoma from the vestibular bulb at the base of the gland can spread to even the mons pubis. Postoperative hematoma is most commonly managed with bed rest, ice packs, and pressure dressings.
■ Chronic pain from gland excision may result from obstructed residual gland or from suture placement. Reoperation may be required at a later point if the introitus is considerably narrowed, wherein vestibulectomy or scar revision may be necessary
Nhận xét
Đăng nhận xét