Ectopic Pregnancy
INTRODUCTION
Ectopic pregnancy is the leading cause of pregnancy-related deaths during the first trimester (1).
The incidence of ectopic pregnancy has been on the increase over the past several decades (2)
and it continues to contribute significantly to maternal morbidity and mortality, especially in the
developing world (3).
Thai ngoài tử cung (TNTC) là nguyên nhân hàng đầu gây tử vong mẹ ở tam cá nguyệt I (1). Tỉ lệ
TNTC ngày càng tăng so với những thập niên trước (2), góp phần đáng kể vào bệnh suất và tử
suất của người mẹ, đặc biệt ở những nước đang phát triển (3).
TNTC ngày càng tăng so với những thập niên trước (2), góp phần đáng kể vào bệnh suất và tử
suất của người mẹ, đặc biệt ở những nước đang phát triển (3).
RISK FACTORS
Several risk factors for ectopic pregnancy exist (4) and are listed in Table 13.1. History of tubal
surgery such as prior tubal sterilization or prior tubal surgery for ectopic pregnancy are amongst
the most common risk factors and thus should heighten alertness for the presence of an ectopic
pregnancy in symptomatic patients. Other risk factors include pelvic inflammatory disease,
female infertility and use of an intra-uterine device.
Các yếu tố nguy cơ của TNTC được liệt kê trong Bảng 13.1 (4). Tiền căn phẫu thuật ống dẫn
trứng (triệt sản) hoặc TNTC trước đó là những yếu tố nguy cơ thường gặp nhất, do đó ở những
bệnh nhân này cần nghĩ ngay đến TNTC khi có triệu chứng nghi ngờ. Những yếu tố nguy cơ
khác bao gồm viêm nhiễm vùng chậu, hiếm muộn và đặt dụng cụ tử cung.
trứng (triệt sản) hoặc TNTC trước đó là những yếu tố nguy cơ thường gặp nhất, do đó ở những
bệnh nhân này cần nghĩ ngay đến TNTC khi có triệu chứng nghi ngờ. Những yếu tố nguy cơ
khác bao gồm viêm nhiễm vùng chậu, hiếm muộn và đặt dụng cụ tử cung.
TABLE 13.1 Risk Factors for Ectopic Pregnancy
- History of tubal surgery
- History of prior ectopic pregnancy
- Use of Intrauterine Device
- History of infertility
Bảng 13.1 Yếu tố nguy cơ TNTC
- Tiền căn phẫu thuật ống dẫn trứng
- Tiền căn TNTC trước đó
- Đặt dụng cụ tử cung
- Tiền căn hiếm muộn
CLINICAL SYMPTOMS
Ectopic pregnancy should be considered when a patient presents with pain and/or vaginal
bleeding in the setting of a positive pregnancy test. The presence of an adnexal mass on physical
examination should also initiate an ectopic pregnancy work-up, when a positive pregnancy test is
present. Clinical symptoms are not specific for ectopic pregnancy and should not be used solely
for diagnosis. The location of the pain may vary (5) and the clinical triad of pain, bleeding and
adnexal mass is present in less than half of patients with ectopic pregnancy (6).
Cần nghĩ đến thai ngoài tử cung trong trường hợp bệnh nhân thử thai dương tính đến khám vì
đau bụng, ra huyết âm đạo hoặc sờ thấy một khối cạnh tử cung. Các triệu chứng lâm sàng không
đặc hiệu cho TNTC do đó không nên dùng đơn thuần để chẩn đoán. Vị trí đau có thể rất khác
nhau (5) và bệnh nhân TNTC có tam chứng kinh điển gồm đau bụng, rong huyết và khối cạnh tử
cung chiếm tỉ lệ < 50% (6).
đau bụng, ra huyết âm đạo hoặc sờ thấy một khối cạnh tử cung. Các triệu chứng lâm sàng không
đặc hiệu cho TNTC do đó không nên dùng đơn thuần để chẩn đoán. Vị trí đau có thể rất khác
nhau (5) và bệnh nhân TNTC có tam chứng kinh điển gồm đau bụng, rong huyết và khối cạnh tử
cung chiếm tỉ lệ < 50% (6).
ANATOMIC LOCATION OF ECTOPIC PREGNANCY
VỊ TRÍ GIẢI PHẪU CỦA TNTC
Most ectopic pregnancies are located along the course of the fallopian tube, with the ampullary
and isthmic sections of the tube accounting for the largest proportions of ectopic pregnancies
(Figure 13.1). Other rare tubal locations include the fimbrial end of the tube or the interstitial
(cornual) end of the tube (Figure 13.1). The interstitial or cornual ectopic pregnancy deserves
special mention, as ectopic pregnancies in this location typically present at a more advanced
stage in gestation and are commonly associated with severe hemorrhage and maternal shock at
the time of presentation.
Hầu hết TNTC làm tổ dọc theo lộ trình của ống dẫn trứng với đoạn bóng và eo chiếm tỉ lệ cao
nhất (Hình 13.1). Những vị trí khác hiếm gặp hơn như loa vòi hoặc đoạn kẽ (đoạn sừng) (Hình
13.1). TNTC đoạn kẽ là dạng đặc biệt bởi vì thai ở vị trí này có thể phát triển lớn và khi vỡ gây
mất máu trầm trọng dẫn đến sốc.
Cornual ectopic pregnancies are also more difficult to diagnose by
ultrasound as they mimic a normal intrauterine gestation, especially when they present at an
advanced stage. Figure 13.2 and 13.3 show cornual ectopic pregnancies in the early part of the
first trimester and Figures 13.4 and 13.5 show cornual ectopic pregnancies at more advanced
gestations. Cervical ectopic pregnancies occur in less than 1 % of all ectopic pregnancies and are
typically diagnosed by transvaginal ultrasound (Figure 13.6). Cervical ectopic pregnancies are
best treated with either intramuscular or direct injection, into the gestational sac, of methotrexate
or potassium chloride (into gestational sac) under ultrasound guidance, especially when
preservation of fertility is desired. Conservative management, following injection of
methotrexate or potassium chloride into the gestational sac, is desired, as long as the patient is
not bleeding excessively, as most injected cervical ectopic pregnancies will spontaneously
resolve.
Thai ở đoạn kẽ khó chẩn đoán trên siêu âm vì rất giống với thai
kì bình thường. Hình 13.2 và 13.3 cho thấy TNTC đoạn kẽ ở giai đoạn sớm của tam cá nguyệt I,
Hình 13.4 và 13.5 cho thấy TNTC đoạn kẽ ở giai đoạn muộn hơn. TNTC ở cổ tử cung chiếm
<1% và được chẩn đoán chủ yếu bằng siêu âm qua ngả âm đạo (Hình 13.6). Thai ở cổ tử cung
được điều trị tốt nhất bằng Methotrexate hoặc potassium chloride tiêm bắp hoặc tiêm trực tiếp
vào túi thai dưới hướng dẫn của siêu âm, đặc biệt trong trường hợp mong muốn bảo tồn khả năng
sinh sản. Sau điều trị cần theo dõi sát bệnh nhân cho đến khi không còn chảy máu nhiều, hầu hết
các thai được tiêm sẽ thoái triển.
In low-resource settings where treatment options are limited, cervical ectopic pregnancy
with heavy vaginal bleeding can be temporarily managed (tamponade) with placement of a
cervical cerclage when technically feasible or by inserting compression (30 cc) Foley ballooncatheter(s) into the cervical canal.
Ở những nơi có nguồn nhân lực thấp, việc điều trị còn hạn chế
thì thai ở cổ tử cung chảy máu nhiều có thể xử trí tạm thời bằng khâu vòng cổ tử cung hoặc đặt
bóng chèn (30cc) với ống thông Foley vào kênh cổ tử cung.
thì thai ở cổ tử cung chảy máu nhiều có thể xử trí tạm thời bằng khâu vòng cổ tử cung hoặc đặt
bóng chèn (30cc) với ống thông Foley vào kênh cổ tử cung.

Figure 13.1: Locations of ectopic pregnancies in the pelvis. Most ectopic pregnancies are
located along the course of the fallopian tube, with the ampullary and isthmic sections
accounting for the largest proportions. Abdominal pregnancy is not depicted in this sketch.
Sketch is courtesy of Dr. Igor Palahnuk.
Hình 13.1: Vị trí TNTC ở vùng chậu. Hầu hết TNTC ở ống dẫn trứng, với đoạn bóng và đoạn eo
chiếm tỉ lệ cao nhất. Thai trong ổ bụng không được mô tả trên hình.
Nguồn: Dr. Igor Palahnuk
chiếm tỉ lệ cao nhất. Thai trong ổ bụng không được mô tả trên hình.
Nguồn: Dr. Igor Palahnuk
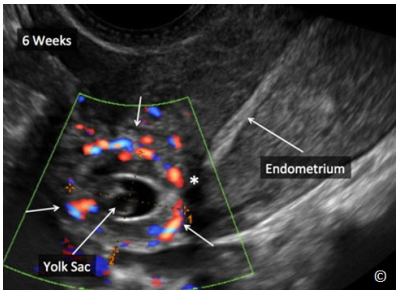
Figure 13.2: Grey scale and color Doppler ultrasound of a cornual ectopic
pregnancy at 6 weeks’ gestation (arrows). Note that the endometrial echo (labeled
as endometrium) is distinctly separate from the cornual ectopic pregnancy
(asterisk). Note the yolk sac within the ectopic pregnancy (labeled).
Hình 13.2: Siêu âm trắng đen và siêu âm Doppler màu TNTC ở đoạn kẽ khoảng 6
tuần với túi noãn hoàng bên trong (mũi tên). Nội mạc tử cung tách biệt với khối
thai (dấu hoa thị).

Figure 13.3: Grey scale ultrasound of a cornual ectopic pregnancy at 7 weeks’
gestation (arrows). Note that the endometrial echo (labeled endometrium) is
distinctly separate from the cornual ectopic pregnancy (asterisk).
Hình 13.3: Siêu âm trắng đen TNTC ở đoạn kẽ khoảng 7 tuần (mũi tên). Nội mạc tử cung tách biệt
với khối thai (dấu hoa thị).
với khối thai (dấu hoa thị).

Figure 13.4: Transvaginal ultrasound of a transverse plane of the upper uterus
showing a cornual ectopic pregnancy (white arrows) at 9 weeks’ gestation. Note
that the endometrial echo (labeled as endometrium) is distinctly separate from
the cornual ectopic pregnancy (asterisk). The ectopic sac is bulging on the
serosal aspect of the uterus (red arrow heads).
Hình 13.4: Siêu âm qua ngã âm đạo với mặt cắt ngang phần trên tử cung cho
thấy TNTC ở đoạn kẽ khoảng 9 tuần (mũi tên trắng). Nội mạc tử cung tách biệt
với khối thai (dấu hoa thị). Túi thai phồng ra bên ngoài lớp thanh mạc tử cung
(mũi tên đỏ).
thấy TNTC ở đoạn kẽ khoảng 9 tuần (mũi tên trắng). Nội mạc tử cung tách biệt
với khối thai (dấu hoa thị). Túi thai phồng ra bên ngoài lớp thanh mạc tử cung
(mũi tên đỏ).

Figure 13.5: Transvaginal ultrasound of an oblique plane of the upper uterus showing a
cornual ectopic pregnancy (arrows) at 13 weeks’ gestation. Note the size of the cornual
pregnancy (labeled) that may be mistaken for an intrauterine gestation. The uterus is
labeled in yellow.
Hình 13.5: Siêu âm qua ngả âm đạo với mặt cắt chếch phần trên tử cung cho thấy TNTC ở
đoạn kẽ khoảng 13 tuần (mũi tên). Kích thước thai giai đoạn này có thể gây nhầm lẫn với
thai trong tử cung
đoạn kẽ khoảng 13 tuần (mũi tên). Kích thước thai giai đoạn này có thể gây nhầm lẫn với
thai trong tử cung
Implantation of a gestational sac in a cesarean section scar is referred to as cesarean scar
implantation and is technically not an ectopic pregnancy as the gestational sac is within the
uterine cavity. Cesarean scar implantation can lead, later in gestation, to severe placental
abnormalities, such as placenta accreta, or rupture of the gestational sac (7, 8).
Thai làm tổ ở sẹo mổ lấy thai về nguyên tắc không phải là TNTC vì túi thai vẫn nằm trong buồng
tử cung. Thai bám ở sẹo mổ lấy thai có thể dẫn đến những bất thường bánh nhau nghiêm trọng ở
giai đoạn muộn của thai kì như nhau cài răng lược hoặc vỡ tử cung (7,8) .
tử cung. Thai bám ở sẹo mổ lấy thai có thể dẫn đến những bất thường bánh nhau nghiêm trọng ở
giai đoạn muộn của thai kì như nhau cài răng lược hoặc vỡ tử cung (7,8) .
The diagnosis of a
cesarean section scar implantation is performed when a gestational sac is noted by ultrasound to
be located in the lower uterine segment, in or near, a cesarean section scar, in a patient with a
prior cesarean section. Magnification of the ultrasound image may help confirm the diagnosis
(Figure 13.7 and 13.8). Similar to cervical ectopic pregnancy, treatment of cesarean section scar
implantation is best achieved by direct injection of methotrexate or potassium chloride into the
gestational sac, under ultrasound guidance (Figure 13.9 A and B).
Ở những sản phụ có
mổ lấy thai trước đó, chẩn đoán thai bám ở sẹo mổ lấy thai cần được nghĩ đến khi siêu âm thấy
túi thai nằm ở phần thấp của tử cung, nằm trong hoặc gần sẹo mổ lấy thai. Việc phóng đại hình
ảnh siêu âm có thể giúp chẩn đoán xác định (Hình 13.7 và 13.8). Tương tự như TNTC ở cổ tử
cung, điều trị thai bám vết mổ cũ đáp ứng tốt nhất với tiêm trực tiếp Methotrexate hoặc
potassium chloride vào túi thai dưới hướng dẫn của siêu âm (Hình 13.9 A và B)
mổ lấy thai trước đó, chẩn đoán thai bám ở sẹo mổ lấy thai cần được nghĩ đến khi siêu âm thấy
túi thai nằm ở phần thấp của tử cung, nằm trong hoặc gần sẹo mổ lấy thai. Việc phóng đại hình
ảnh siêu âm có thể giúp chẩn đoán xác định (Hình 13.7 và 13.8). Tương tự như TNTC ở cổ tử
cung, điều trị thai bám vết mổ cũ đáp ứng tốt nhất với tiêm trực tiếp Methotrexate hoặc
potassium chloride vào túi thai dưới hướng dẫn của siêu âm (Hình 13.9 A và B)

Figure 13.6: Transvaginal ultrasound of a sagittal plane of the uterus showing a cervical
ectopic pregnancy (arrows). The uterine fundus and cervix are labeled for image orientation.
Hình 13.6: Siêu âm qua ngả âm đạo mặt cắt dọc tử cung cho thấy TNTC ở cổ tử cung

Figure 13.7: Transvaginal ultrasound in grey scale of a sagittal plane of the uterus showing a
cesarean scar implantation of a gestational sac (arrows). The cervix is labeled for image
orientation.
Hình 13.7: Siêu âm trắng đen qua ngả âm đạo với mặt cắt dọc tử cung cho thấy thai bám ở
sẹo mổ lấy thai (mũi tên).
sẹo mổ lấy thai (mũi tên).

Figure 13.8: Transvaginal ultrasound in color Doppler of a sagittal plane of the uterus showing
a cesarean scar implantation of a gestational sac (arrows – same as in figure 13.7). Note the
increased vascularity on color Doppler of the gestational sac. The cervix is labeled for image
orientation.
Hình 13.8: Siêu âm Doppler màu qua ngả âm đạo với mặt cắt dọc tử cung cho thấy thai bám ở
sẹo mổ lấy thai và có tăng sinh mạch máu trên Doppler màu.
sẹo mổ lấy thai và có tăng sinh mạch máu trên Doppler màu.
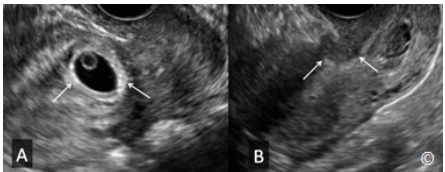
Figure 13.9 A and B: Transvaginal ultrasound of a sagittal plane of the uterus showing in (A)
a cesarean scar implantation (arrows). The figure B shows the same cesarean scar
implantation (arrows) two weeks after direct methotrexate injection. Note the significant
resolution.
Hình 13.9 A và B: Siêu âm qua ngả âm đạo với mặt cắt dọc tử cung:
Hình A: thai bám ở sẹo mổ lấy thai
Hình B: túi thai này thoái triển đáng kể sau 2 tuần tiêm Methotrexate trực tiếp
Hình A: thai bám ở sẹo mổ lấy thai
Hình B: túi thai này thoái triển đáng kể sau 2 tuần tiêm Methotrexate trực tiếp
STEP-WISE ULTRASOUND APPROACH TO THE DIAGNOSIS OF ECTOPIC
PREGNANCY
CÁC BƯỚC TIẾP CẬN TRONG SIÊU ÂM CHẨN ĐOÁN TNTC
This section describes the step-wise approach to the work-up of a woman presenting with clinical
symptoms suggestive of the presence of an ectopic pregnancy. Before this stepwise approach is
initiated, it is important to note that taking a detailed history and performing a physical
examination are essential components of the care of the woman and thus should be part of the
initial evaluation. A differential diagnosis should then be formulated as new information and
diagnostic tests are being gathered. Table 13.2 lists a typical differential diagnosis for a woman
presenting with lower abdominal pain and vaginal bleeding.
Phần này mô tả các bước tiếp cận một bệnh nhân nữ đến khám với triệu chứng lâm sàng nghi
ngờ TNTC. Việc khai thác chi tiết bệnh sử và khám lâm sàng rất cần thiết để đánh giá ban đầu
bệnh nhân. Kết hợp các triệu chứng lâm sàng và xét nghiệm để đưa ra các chẩn đoán phù hợp.
Bảng 13.2 liệt kê các chẩn đoán phân biệt ở bệnh nhân nữ có triệu chứng đau bụng dưới và ra
huyết âm đạo
ngờ TNTC. Việc khai thác chi tiết bệnh sử và khám lâm sàng rất cần thiết để đánh giá ban đầu
bệnh nhân. Kết hợp các triệu chứng lâm sàng và xét nghiệm để đưa ra các chẩn đoán phù hợp.
Bảng 13.2 liệt kê các chẩn đoán phân biệt ở bệnh nhân nữ có triệu chứng đau bụng dưới và ra
huyết âm đạo
TABLE 13.2
Differential Diagnosis of a Woman Presenting in the Reproductive Age
Group with Lower Abdominal Pain and Vaginal Bleeding
- Normal pregnancy
- Threatened or impending miscarriage
- Ectopic pregnancy
- Symptomatic ovarian mass (hemorrhagic cyst, dermoid, torsion)
- Pelvic inflammatory disease
- Abnormal uterine bleeding
- Gastrointestinal origin
- Urinary origin
Bảng 13.2
Các chẩn đoán phân biệt ở một phụ nữ trong độ tuổi sinh sản có triệu
chứng đau bụng dưới và ra huyết âm đạo
- Thai kì bình thường
- Dọa sẩy thai
- Thai ngoài tử cung
- Khối u buồng trứng (nang xuất huyết, u bì, u buồng trứng xoắn)
- Bệnh lý viêm nhiễm vùng chậu
- Xuất huyết tử cung bất thường
- Nguyên nhân từ đường tiêu hóa
- Nguyên nhân từ đường tiết niệu
Obtaining a pregnancy test should be one of the first diagnostic tests to be performed. A negative
pregnancy test practically rules out a live ectopic pregnancy, assuming that the pregnancy test
that is available has sufficient sensitivity to detect human chorionic gonadotropin (HCG) levels
commensurate with early pregnancy. A positive pregnancy test establishes pregnancy but does
not indicate the location of the gestational sac, or the viability of the pregnancy. Please note that
chronic ectopic pregnancies may coexist with low HCG levels and are typically associated with
chronic pelvic pain. Figures 13.10 and 13.11 show a chronic ectopic pregnancy with an HCG
level of 22 IU / ml. The patient presented with a pelvic mass and chronic right pelvic pain.
Thử thai là một trong những xét nghiệm chẩn đoán đầu tiên cần được thực hiện. Thử thai âm tính
gần như giúp loại trừ TNTC sống (lưu ý xét nghiệm này phải có độ nhạy cao với nồng độ HCG
(Human Chorionic Gonadotropin) ở thai giai đoạn sớm). Xét nghiệm dương tính xác nhận có
thai nhưng không cho biết vị trí hoặc khả năng sống của thai. Cần chú ý những trường hợp
TNTC mạn tính với nồng độ HCG thấp kèm theo triệu chứng đau vùng chậu mạn tính. Hình
13.10 và 13.11 minh họa TNTC mạn tính với nồng độ HCG là 22 IU/ml, bệnh nhân có triệu
chứng đau vùng chậu phải mạn tính và khám thấy một khối ở vùng chậu.

Figure 13.10: Transvaginal ultrasound showing a chronic ectopic pregnancy (arrowsconfirmed on pathology) in a woman who presented with chronic pelvic pain. HCG levels
were 22 IU/ml. A separate ovary was noted (labeled). The uterus (labeled) is seen adjacent to
the chronic ectopic.
Hình 13.10: Siêu âm qua ngả âm đạo: TNTC mạn tính ở 1 phụ nữ có triệu chứng đau vùng
chậu mạn tính (mũi tên - đã được kiểm chứng bằng giải phẫu bệnh). Nồng độ HCG 22 IU/ml.

Figure 13.11: Transvaginal ultrasound with color Doppler in the same woman as in figure
13.10 showing significant vascularity of the chronic ectopic pregnancy (arrows)
Hình 13.11: Siêu âm Doppler màu qua ngả âm đạo trên cùng người phụ nữ trong hình 13.10
cho thấy có tăng sinh mạch máu ở khối TNTC mạn tính
cho thấy có tăng sinh mạch máu ở khối TNTC mạn tính
Given that this textbook represents a basic approach to the use of ultrasound in obstetrics and
gynecology, we will not expand on the relationship of the serum HCG level with the sonographic
appearance of the gestational sac in the uterus. Suffice it to say that there is a relationship
between rising HCG levels and normal intrauterine pregnancies.
In general, normal pregnancies
will show a doubling of the HCG level every 2-3 days (9). This rule however is not exclusive as
1 in 5 ectopic pregnancies will show this rise in HCG levels (9) and thus HCG levels should not
be used alone in excluding an ectopic pregnancy.
Trong phạm vi cuốn sách này chỉ trình bày cách tiếp cận cơ bản về việc sử dụng siêu âm trong
sản phụ khoa, chúng tôi sẽ không đề cập đến mối tương quan của nồng độ HCG trong huyết
thanh với hình ảnh siêu âm của túi thai trong tử cung. Thông thường, nồng độ HCG tăng gấp đôi
mỗi 2 – 3 ngày ở thai kì bình thường (9). Tuy nhiên quy luật này không đúng tuyệt đối vì có
khoảng 20% trường hợp TNTC sẽ có biểu hiện tăng nồng độ HCG như trên (9) do đó không nên
dùng nồng độ HCG đơn thuần để loại trừ TNTC.
sản phụ khoa, chúng tôi sẽ không đề cập đến mối tương quan của nồng độ HCG trong huyết
thanh với hình ảnh siêu âm của túi thai trong tử cung. Thông thường, nồng độ HCG tăng gấp đôi
mỗi 2 – 3 ngày ở thai kì bình thường (9). Tuy nhiên quy luật này không đúng tuyệt đối vì có
khoảng 20% trường hợp TNTC sẽ có biểu hiện tăng nồng độ HCG như trên (9) do đó không nên
dùng nồng độ HCG đơn thuần để loại trừ TNTC.
The stepwise ultrasound approach hereby described should be initiated if the pregnancy test is
positive.
This stepwise approach is performed by the transvaginal ultrasound:
Vì vậy việc tiếp cận siêu âm theo bước nên được tiến hành nếu xét nghiệm thử thai dương tính.
Cách tiếp cận này được áp dụng khi siêu âm ngả âm đạo:
Cách tiếp cận này được áp dụng khi siêu âm ngả âm đạo:
Step one:
Assess the endometrial cavity for the presence of a gestational sac:
Đánh giá sự hiện diện của túi thai trong buồng tử cung:
The presence of a gestational sac in the endometrial cavity (Figure 13.12) practically rules out
an ectopic pregnancy. Note that on very rare occasions, a heterotopic pregnancy can occur (a
concurrent intrauterine and an extrauterine pregnancy) (Figure 13.13) – (Clip 13.1). The
incidence of a heterotopic pregnancy in a natural pregnancy is around 1 in 7000 pregnancies.
Heterotopic pregnancies are more common in pregnancies of assisted reproduction (Figure
13.14).
Sự hiện diện của túi thai trong buồng tử cung giúp loại trừ TNTC trong phần lớn các trường hợp
(Hình 13.12). Tuy rất hiếm gặp nhưng cũng có khả năng một thai trong kết hợp với một thai
ngoài tử cung (heterotopic pregnancy) (Hình 13.13) – (Clip 13.1). Tỉ lệ thai trong – thai ngoài tử
cung trong thai kì tự nhiên vào khoảng 1/7000 và thường gặp hơn ở những trường hợp được thực
hiện các kĩ thuật hỗ trợ sinh sản (Hình 13.14).
(Hình 13.12). Tuy rất hiếm gặp nhưng cũng có khả năng một thai trong kết hợp với một thai
ngoài tử cung (heterotopic pregnancy) (Hình 13.13) – (Clip 13.1). Tỉ lệ thai trong – thai ngoài tử
cung trong thai kì tự nhiên vào khoảng 1/7000 và thường gặp hơn ở những trường hợp được thực
hiện các kĩ thuật hỗ trợ sinh sản (Hình 13.14).
The gestational sac of a normal pregnancy on ultrasound, which appears between the 4th and the
5th menstrual week, corresponds to the chorionic cavity of the embryo (Figure 13.12). The yolk
sac is the first structure to appear on ultrasound within the gestational sac and is typically first
seen at the 5th menstrual week (Figure 13.15), followed by the amnion between the 5th and the
6th week and the embryo by the 6th menstrual week (Figure 13.16). The normal intrauterine
gestational sac has a distinctive ultrasound appearance, with a thick rim of echogenic tissue
(Figure 13.17). This echogenic rim differentiates the gestational sac from blood or fluid
collection within the endometrial cavity. Blood or fluid collection within the endometrial cavity
is commonly called pseudosac (Figure 13-18 A and B). The term pseudosac is used in relation
to the presence of an ectopic pregnancy. For more discussion on the first trimester, please refer to
chapter 4.
Ở thai kì bình thường túi thai xuất hiện khoảng giữa tuần thứ 4 và thứ 5, đó là khoang màng đệm
của phôi thai (Hình 13.12). Túi noãn hoàng (Yolk sac) là cấu trúc đầu tiên có thể thấy được trên
siêu âm lúc thai 5 tuần (Hình 13.15), kế đến là khoang ối xuất hiện khoảng giữa tuần thứ 5 và
thứ 6, và phôi thai xuất hiện lúc 6 tuần (Hình 13.16). Trên siêu âm, túi thai bình có bờ dày sáng
(Hình 13.17). Bờ phản âm dày này giúp phân biệt túi thai với tụ máu hoặc dịch trong lòng tử
cung. Tụ máu hoặc tụ dịch trong lòng tử cung thường được gọi là túi thai giả (Hình 13-18 A và
B). Thuật ngữ túi thai giả được dùng trong mối tương quan với TNTC. Để bàn luận nhiều hơn về
tam cá nguyệt 1, xin tham khảo chương 4.
của phôi thai (Hình 13.12). Túi noãn hoàng (Yolk sac) là cấu trúc đầu tiên có thể thấy được trên
siêu âm lúc thai 5 tuần (Hình 13.15), kế đến là khoang ối xuất hiện khoảng giữa tuần thứ 5 và
thứ 6, và phôi thai xuất hiện lúc 6 tuần (Hình 13.16). Trên siêu âm, túi thai bình có bờ dày sáng
(Hình 13.17). Bờ phản âm dày này giúp phân biệt túi thai với tụ máu hoặc dịch trong lòng tử
cung. Tụ máu hoặc tụ dịch trong lòng tử cung thường được gọi là túi thai giả (Hình 13-18 A và
B). Thuật ngữ túi thai giả được dùng trong mối tương quan với TNTC. Để bàn luận nhiều hơn về
tam cá nguyệt 1, xin tham khảo chương 4.
If a gestational sac is seen within the endometrial cavity, complete the ultrasound examination by
evaluating the adnexal regions and the cul-de-sac. Go to step 2, if no gestational sac is seen in the
endometrial cavity.
Nếu thấy túi thai trong lòng tử cung, việc khám siêu âm sẽ hoàn tất bằng việc đánh giá phần phụ
và túi cùng. Nếu không thấy túi thai trong lòng tử cung, chúng ta chuyển sang bước 2.
và túi cùng. Nếu không thấy túi thai trong lòng tử cung, chúng ta chuyển sang bước 2.

Figure 13.12: Transvaginal ultrasound of a sagittal plane of the uterus showing a gestational
sac (labeled) at about 5 weeks’ gestation. The presence of an intrauterine gestational sac
practically rules out an ectopic pregnancy with some exceptions. See text for details.
Hình 13.12: Siêu âm qua ngả âm đạo với mặt cắt dọc tử cung cho thấy túi thai khoảng 5 tuần
tuổi. Sự hiện diện túi thai trong lòng tử cung giúp loại trừ TNTC trong phần lớn các trường
hợp.
tuổi. Sự hiện diện túi thai trong lòng tử cung giúp loại trừ TNTC trong phần lớn các trường
hợp.

Figure 13.13: Transvaginal ultrasound of a heterotopic pregnancy at 6 week’s gestation. Note
the presence of an intrauterine pregnancy (IUP) and a tubal ectopic pregnancy (labeled) in
the adnexa.
Hình 13.13: Siêu âm qua ngả âm đạo cho thấy sự hiện diện đồng thời cả thai trong tử cung
(IUP: intrauterine pregnancy) và thai ngoài tử cung # 6 tuần.
(IUP: intrauterine pregnancy) và thai ngoài tử cung # 6 tuần.

Figure 13.14: Transvaginal ultrasound of a heterotopic pregnancy at 7 week’s gestation. Note
the presence of a triplet intrauterine pregnancy (asterisks - Triplet IUPs) and a tubal ectopic
pregnancy (labeled) in the adnexa. This pregnancy was conceived by assisted reproduction.
Hình 13.14: Siêu âm qua ngả âm đạo thai trong – thai ngoài tử cung khoảng 7 tuần tuổi. Hiện
diện tam thai trong tử cung và TNTC ở ống dẫn trứng. Thai kì được thực hiện kĩ thuật hỗ trợ
sinh sản
diện tam thai trong tử cung và TNTC ở ống dẫn trứng. Thai kì được thực hiện kĩ thuật hỗ trợ
sinh sản
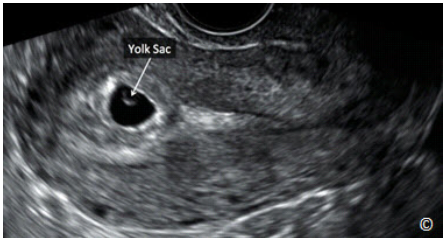
Figure 13.15: Transvaginal ultrasound of a sagittal plane of the uterus showing a gestational
sac at 5 weeks’ gestation with a yolk sac (labeled). Note that the yolk sac is the first structure
to appear within the gestational sac and is typically first seen at the 5th menstrual week.
Hình 13.15: Siêu âm qua ngả âm đạo với mặt cắt dọc tử cung cho thấy túi thai khoảng 5 tuần
có túi noãn hoàng. Túi noãn hoàng là cấu trúc đầu tiên xuất hiện trên siêu âm bên trong túi
thai lúc thai 5 tuần
có túi noãn hoàng. Túi noãn hoàng là cấu trúc đầu tiên xuất hiện trên siêu âm bên trong túi
thai lúc thai 5 tuần
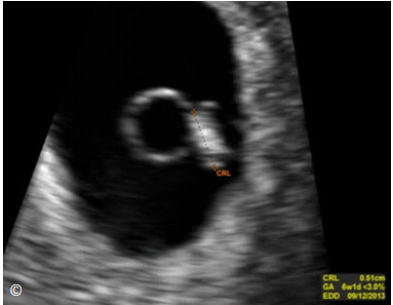
Figure 13.16: Transvaginal ultrasound of a gestational sac at 6 weeks’ gestation showing an
embryo (measured). The yolk sac (not labeled) is seen next to the embryo. CRL = crown rump
length, GA = gestational age and EDD = estimated date of delivery.
Hình 13.16: Siêu âm qua ngả âm đạo cho thấy túi thai 6 tuần đã có phôi thai. Túi noãn hoàng
bên cạnh phôi thai.
bên cạnh phôi thai.

Figure 13.17: Transvaginal ultrasound of a sagittal plane of the uterus with a normal
gestational sac (labeled) at 5 weeks’ gestation. Note the echogenic rim surrounding the
gestational sac (dashed circle).
Hình 13.17: Siêu âm qua ngả âm đạo với mặt cắt dọc tử cung: túi thai bình thường khoảng 5
tuần. Lưu ý có viền phản âm dày quanh túi thai.
tuần. Lưu ý có viền phản âm dày quanh túi thai.

Figure 13.18 A and B: Transvaginal ultrasound of sagittal planes of two uteri (A) and (B) with
endometrial fluid (arrows) in the setting of suspected ectopic pregnancies. The term pseudosac is used
when endometrial fluid is noted in association with an ectopic pregnancy.
Hình 13.18 A và B: Siêu âm qua ngả âm đạo với mặt cắt dọc cho thấy dịch trong lòng tử cung ở những
bệnh nhân nghi ngờ TNTC. Thuật ngữ túi thai giả được dùng để chỉ dịch trong lòng tử cung ở những
trường hợp TNTC.
bệnh nhân nghi ngờ TNTC. Thuật ngữ túi thai giả được dùng để chỉ dịch trong lòng tử cung ở những
trường hợp TNTC.
Step Two:
Assess the cul-de-sac for the presence of fluid:
Đánh giá dịch túi cùng:
The presence of fluid in the cul-de-sac is an important part of this evaluation as it may suggest
the presence of blood from a ruptured ectopic pregnancy or a ruptured ovarian cyst. The cul-desac can be assessed for fluid or blood on ultrasound by imaging the space posterior to the cervix
and the lower uterine segment in a sagittal plane of the uterus and cervix using the transvaginal
approach (Figure 13.19). Low-velocity color Doppler, if available, can be used to confirm the
absence of vascular flow within the blood clots.
Đánh giá dịch túi cùng là một phần quan trọng gợi ý sự hiện diện của máu do TNTC vỡ hoặc
nang buồng trứng vỡ. Túi cùng được giới hạn phía trước bởi phần thấp của tử cung, cổ tử cung
và phía sau bởi trực tràng, việc đánh giá dịch túi cùng được thực hiện qua siêu âm ngã âm đạo
với mặt cắt dọc tử cung (Hình 13.19). Có thể sử dụng Doppler màu với vận tốc thấp để xác nhận
không có dòng chảy của mạch máu bên trong cục máu đông.
nang buồng trứng vỡ. Túi cùng được giới hạn phía trước bởi phần thấp của tử cung, cổ tử cung
và phía sau bởi trực tràng, việc đánh giá dịch túi cùng được thực hiện qua siêu âm ngã âm đạo
với mặt cắt dọc tử cung (Hình 13.19). Có thể sử dụng Doppler màu với vận tốc thấp để xác nhận
không có dòng chảy của mạch máu bên trong cục máu đông.
It is important to note that the mere presence of
fluid in the cul-de-sac in a patient with a suspected ectopic pregnancy should be concerning for
the possibility of intra-abdominal bleeding and this information should be considered in the
overall management of the patient. If fluid is noted in the cul-de-sac region in significant
quantity, assessing the regions in the upper gutters of the abdomen is important as the presence
of fluid in those locations will confirm that a significant amount of free fluid is present in the
abdomen and pelvis and will raise the suspicion for significant intra-peritoneal bleeding. It is
also important to note that the presence of fluid in the cul-de-sac in small amount is a normal
finding and is part of the normal physiologic changes of the menstrual cycle.
Ở bệnh nhân nghi ngờ TNTC, siêu
âm thấy dịch túi cùng thì phải xem xét khả năng có xuất huyết nội và cần kết hợp với đánh giá
tổng trạng bệnh nhân để có hướng xử trí thích hợp. Nếu lượng dịch túi cùng nhiều, chúng ta phải
quan sát những ngách cao hơn của ổ bụng, sự hiện diện của dịch ở những ngách này gợi ý có
chảy máu nhiều trong khoang phúc mạc (Ghi chú của người dịch: Túi cùng (Pouch) là do lá phúc
mạc lách giữa các tạng ở chậu hông tạo thành một túi sâu của phúc mạc. Đây là những nơi thấp
nhất của ổ phúc mạc mà các dịch trong ổ bụng trong các trường hợp bệnh lý thường đọng ở đó.
Trong phần này tác giả sử dụng thuật ngữ Cul-de-sac để chỉ túi cùng Douglas (Douglas’ pouch).
Ngách (Recess) cũng là do lá phúc mạc lách giữa các tạng hay giữa các tạng với thành bụng để
tạo thành một rãnh hoặc một hốc nhưng đó không phải là chỗ thấp nhất của ổ bụng. Ví dụ ngách
dưới gan, ngách gan thận, … Nguồn: Bài giảng Giải Phẫu Học 2006 – ĐHYD TP.HCM – Trang
273-274). Lưu ý rằng bình thường cũng có ít dịch ở túi cùng và đó là dịch sinh lý do sự thay đổi
của chu kỳ kinh.
âm thấy dịch túi cùng thì phải xem xét khả năng có xuất huyết nội và cần kết hợp với đánh giá
tổng trạng bệnh nhân để có hướng xử trí thích hợp. Nếu lượng dịch túi cùng nhiều, chúng ta phải
quan sát những ngách cao hơn của ổ bụng, sự hiện diện của dịch ở những ngách này gợi ý có
chảy máu nhiều trong khoang phúc mạc (Ghi chú của người dịch: Túi cùng (Pouch) là do lá phúc
mạc lách giữa các tạng ở chậu hông tạo thành một túi sâu của phúc mạc. Đây là những nơi thấp
nhất của ổ phúc mạc mà các dịch trong ổ bụng trong các trường hợp bệnh lý thường đọng ở đó.
Trong phần này tác giả sử dụng thuật ngữ Cul-de-sac để chỉ túi cùng Douglas (Douglas’ pouch).
Ngách (Recess) cũng là do lá phúc mạc lách giữa các tạng hay giữa các tạng với thành bụng để
tạo thành một rãnh hoặc một hốc nhưng đó không phải là chỗ thấp nhất của ổ bụng. Ví dụ ngách
dưới gan, ngách gan thận, … Nguồn: Bài giảng Giải Phẫu Học 2006 – ĐHYD TP.HCM – Trang
273-274). Lưu ý rằng bình thường cũng có ít dịch ở túi cùng và đó là dịch sinh lý do sự thay đổi
của chu kỳ kinh.

Figure 13.19: Transvaginal ultrasound of a sagittal plane of the uterus in a patient with a
ruptured ectopic pregnancy. Note the presence of free fluid in the cul-de-sac and surrounding
the uterus (asterisks). A blood clot (labeled) is also noted in the cul-de-sac. In this image, the
endometrial thickness is also measured (yellow calipers).
Hình 13.19: Siêu âm qua ngả âm đạo với mặt cắt dọc tử cung ở bênh nhân TNTC vỡ có dịch tự
do ở túi cùng và xung quanh tử cung (dấu hoa thị). Có hình ảnh cục máu đông ở túi cùng sau
và lớp dịch mỏng trong lòng tử cung.
do ở túi cùng và xung quanh tử cung (dấu hoa thị). Có hình ảnh cục máu đông ở túi cùng sau
và lớp dịch mỏng trong lòng tử cung.
Step 3:
Assess the Adnexal Region for the Ectopic Gestational Sac:
Đánh giá khối TNTC ở khu vực phần phụ:
The third step in the ultrasound examination of the pelvis includes a thorough evaluation of both
adnexal regions in transverse and sagittal scanning planes. This evaluation should include
assessment of the ovaries and the surrounding anatomic regions, looking for fluid, blood and for
the ectopic gestational sac. The ectopic gestational sac, when present in the adnexal region, is
commonly in the fallopian tube. It is typically round in shape and has an echogenic ring and an
anechoic center (Figure 13.20 A and B).
Đánh giá một cách kỹ lưỡng khu vực phần phụ trên cả 2 mặt cắt ngang và dọc. Bước này bao
gồm đánh giá buồng trứng và khu vực xung quanh để tìm dịch, máu và khối TNTC. Khối TNTC
thường nằm ở ống dẫn trứng và điển hình có dạng hình tròn với viền phản âm dày bao quanh túi
phản âm trống (Hình 13.20 A và B).
gồm đánh giá buồng trứng và khu vực xung quanh để tìm dịch, máu và khối TNTC. Khối TNTC
thường nằm ở ống dẫn trứng và điển hình có dạng hình tròn với viền phản âm dày bao quanh túi
phản âm trống (Hình 13.20 A và B).
Commonly, the patient’s symptoms correlate with the
location of the ectopic pregnancy in the pelvis but with noted exceptions. It is also important not
to confuse an ectopic gestational sac with a corpus luteum (Figure 13.21), which is commonly
located on the ovary of the same side as the ectopic. Table 13.3 shows differentiating
characteristics of the corpus luteum from the ectopic gestational sac. Figures 13.22 and 13.23
show tubal ectopic pregnancies on ultrasound. Color Doppler is not helpful in the differential
diagnosis given the overlap with corpus luteum flow and the varying degrees of blood flow
patterns in ectopic pregnancies. Figure 13.24 A-C shows varying degrees of blood flow on color
Doppler in three different ectopic pregnancies.
Thông thường triệu chứng lâm sàng của bệnh nhân có liên
quan với vị trí của khối TNTC nhưng cũng có trường hợp ngoại lệ. Điều quan trọng nữa là không
được nhầm lẫn khối TNTC với nang hoàng thể (Hình 13.21), nó thường nằm ở buồng trứng
cùng bên với khối TNTC. Bảng 13.3 thể hiện những đặc tính phân biệt nang hoàng thể với khối
TNTC. Hình 13.22 và 13.23 cho thấy khối TNTC ở ống dẫn trứng trên siêu âm. Dấu hiệu tăng
sinh mạch máu nhiều trên siêu âm Doppler màu của nang hoàng thể không giúp phân biệt với
khối TNTC vì khối TNTC có nhiều mức độ tăng sinh mạch máu khác nhau. Hình 13.24 A-C cho
thấy mức độ dòng chảy khác nhau trên siêu âm Doppler ở 3 trường hợp TNTC khác nhau
quan với vị trí của khối TNTC nhưng cũng có trường hợp ngoại lệ. Điều quan trọng nữa là không
được nhầm lẫn khối TNTC với nang hoàng thể (Hình 13.21), nó thường nằm ở buồng trứng
cùng bên với khối TNTC. Bảng 13.3 thể hiện những đặc tính phân biệt nang hoàng thể với khối
TNTC. Hình 13.22 và 13.23 cho thấy khối TNTC ở ống dẫn trứng trên siêu âm. Dấu hiệu tăng
sinh mạch máu nhiều trên siêu âm Doppler màu của nang hoàng thể không giúp phân biệt với
khối TNTC vì khối TNTC có nhiều mức độ tăng sinh mạch máu khác nhau. Hình 13.24 A-C cho
thấy mức độ dòng chảy khác nhau trên siêu âm Doppler ở 3 trường hợp TNTC khác nhau

Figure 13.20 A and B: Tubal ectopic pregnancies in A and B (arrows) imaged on transvaginal
ultrasound. Note the echogenic ring and the anechoic center (doughnut-like appearance) in both
ectopic pregnancies. Color Doppler in B shows moderate ectopic sac vascularity. The ovary is seen
(labeled) in A.
Hình 13.20 A và B: Siêu âm qua ngả âm đạo: TNTC ở ống dẫn trứng. Hình ảnh vòng phản âm dày và
trung tâm phản âm trống (dấu hiệu doughnut). Hình B cho thấy khối TNTC tăng sinh mạch máu mức
độ trung bình trên siêu âm Doppler màu.
trung tâm phản âm trống (dấu hiệu doughnut). Hình B cho thấy khối TNTC tăng sinh mạch máu mức
độ trung bình trên siêu âm Doppler màu.

Figure 13.21: Transvaginal ultrasound in grey scale and color Doppler of a corpus luteum (arrows)
within the ovary (labeled). See Table 13.3 for differentiating features from an ectopic pregnancy.
Hình 13.21: Siêu âm trắng đen và siêu âm Doppler màu ngã âm đạo: nang hoàng thể bên trong
buồng trứng. Xem những dầu hiện phân biệt với TNTC ở Bảng 13.3.
buồng trứng. Xem những dầu hiện phân biệt với TNTC ở Bảng 13.3.
TABLE 13.3 Differentiating Features of a Corpus Luteum From an Ectopic Pregnancy
- Corpus luteum is located within the ovary
- Corpus luteum is surrounded by normal ovarian tissue
- Corpus luteum moves with the ovary with manipulation
- Corpus luteum typically does not have a thick echogenic ring
- Color Doppler and pulsed Doppler cannot differentiate between the two entities
BẢNG 13.3 Những dấu hiệu phân biệt nang hoàng thể và TNTC
- Nang hoàng thể nằm ở buồng trứng
- Nang hoàng thể được bao bọc xung quanh bởi mô buồng trứng bình thường
- Nang hoàng thể di chuyển cùng với buồng trứng khi làm nghiệm pháp đẩy đầu dò
- Nang hoàng thể điển hình không có vòng phản âm dày
- Siêu âm Doppler màu và Doppler xung không phân biệt được 2 cấu trúc này
- Nang hoàng thể nằm ở buồng trứng
- Nang hoàng thể được bao bọc xung quanh bởi mô buồng trứng bình thường
- Nang hoàng thể di chuyển cùng với buồng trứng khi làm nghiệm pháp đẩy đầu dò
- Nang hoàng thể điển hình không có vòng phản âm dày
- Siêu âm Doppler màu và Doppler xung không phân biệt được 2 cấu trúc này

Figure 13.22: Transvaginal ultrasound showing a tubal ectopic pregnancy (arrows). Note the
separation of the ectopic sac from the ovary (labeled). The ectopic sac has echogenic borders and an
anechoic center (doughnut-like appearance).
Hình 13.22: Siêu âm qua ngả âm đạo: TNTC ở ống dẫn trứng. Khối TNTC tách biệt với buồng trứng.
Khối TNTC có bờ phản âm dày và trung tâm phản âm trống (dấu hiệu doughnut)
Khối TNTC có bờ phản âm dày và trung tâm phản âm trống (dấu hiệu doughnut)

Figure 13.23: Transvaginal ultrasound showing a tubal ectopic pregnancy (arrows). Note the
echogenic thick borders and an anechoic center (doughnut-like appearance). The ovary is
labeled and is typically lateral to the ectopic gestation.
Hình 13.23: Siêu âm qua ngả âm đạo: TNTC ở ống dẫn trứng. Khối TNTC có bờ phản âm dày và
trung tâm phản âm trống (dấu hiệu doughnut).
trung tâm phản âm trống (dấu hiệu doughnut).

Figure 13.24 A, B, and C: Tubal ectopic pregnancies in A, B and C (arrows) imaged on transvaginal
ultrasound with color Doppler at similar velocity scale and filter set-up. Note the varying degrees of
vascularity between ectopic pregnancies with minimal to absent in A, moderate in B and excessive in C.
Color Doppler is not a helpful differentiating feature of ectopic pregnancy.
Hình 13.24 A, B, và C: Hình ảnh TNTC ở ống dẫn trứng trên siêu âm Doppler màu ngã âm đạo với vận tốc
dòng chảy và độ lọc thành giống nhau: rất thấp hoặc không có ở hình A, mức độ trung bình ở hình B, và
mức độ nhiều ở hình C. Siêu âm Doppler màu không giúp ích cho việc chẩn đoán phân biệt TNTC và nang
hoàng thể.
dòng chảy và độ lọc thành giống nhau: rất thấp hoặc không có ở hình A, mức độ trung bình ở hình B, và
mức độ nhiều ở hình C. Siêu âm Doppler màu không giúp ích cho việc chẩn đoán phân biệt TNTC và nang
hoàng thể.
The presence of an ectopic gestational sac in the adnexa that is distinctly separate from the ovary
in a woman presenting with symptoms suggestive of an ectopic pregnancy, especially in the
absence of an intra-uterine gestational sac, establishes the diagnosis of an ectopic pregnancy. The
additional presence of fluid in the cul-de-sac confirms the diagnosis. When ultrasound findings
are not diagnostic of ectopic pregnancy, it is important to consider all findings and make a
judgment based upon available information. Given that significant change in the normal
gestation occurs in the first trimester in a short time-frame, a follow-up ultrasound within a short
period of time such as in 3 to 4 days when the woman’s medical condition is stable and
compliance is adequate, may help clarify the diagnosis. If the woman’s condition is unstable,
intervention is warranted irrespective of the ultrasound findings.
Đứng trước một phụ nữ có triệu chứng gợi ý TNTC, siêu âm thấy khối TNTC ở phần phụ nằm
tách biệt với buồng trứng và không thấy túi thai trong tử cung cần nghĩ ngay đến bệnh cảnh
TNTC. Sự hiện diện dịch ở túi cùng sau giúp xác nhận chẩn đoán. Trong trường hợp những dấu
hiệu siêu âm không gợi ý chẩn đoán TNTC, cần phải xem xét tất cả các xét nghiệm và đưa ra
chẩn đoán dựa trên những thông tin có sẵn. Có nhiều sự thay đổi xảy ra trong thời gian ngắn ở
thai kì bình thường trong tam cá nguyệt I nên việc siêu âm lập lại trong khoảng 3 đến 4 ngày đối
với bệnh nhân có tình trạng lâm sàng ổn định và tuân thủ đúng sẽ giúp làm sáng tỏ chẩn đoán.
Nếu tình trạng bệnh nhân không ổn định, việc điều trị can thiệp được phép thực hiện mà không
cần đến những dấu hiệu siêu âm.
tách biệt với buồng trứng và không thấy túi thai trong tử cung cần nghĩ ngay đến bệnh cảnh
TNTC. Sự hiện diện dịch ở túi cùng sau giúp xác nhận chẩn đoán. Trong trường hợp những dấu
hiệu siêu âm không gợi ý chẩn đoán TNTC, cần phải xem xét tất cả các xét nghiệm và đưa ra
chẩn đoán dựa trên những thông tin có sẵn. Có nhiều sự thay đổi xảy ra trong thời gian ngắn ở
thai kì bình thường trong tam cá nguyệt I nên việc siêu âm lập lại trong khoảng 3 đến 4 ngày đối
với bệnh nhân có tình trạng lâm sàng ổn định và tuân thủ đúng sẽ giúp làm sáng tỏ chẩn đoán.
Nếu tình trạng bệnh nhân không ổn định, việc điều trị can thiệp được phép thực hiện mà không
cần đến những dấu hiệu siêu âm.
A rare presentation of an ectopic pregnancy is the abdominal pregnancy. Abdominal pregnancy
can be associated with significant morbidity, especially if the pregnancy is allowed to grow.
Placental insertion on the bowels or pelvic vasculature can result in significant bleeding if
removal is attempted. If an advanced abdominal pregnancy is encountered, it is prudent to
remove the fetus but keep the placenta in situ to avoid massive bleeding. Figures 13.25 and
13.26 show an abdominal pregnancy at 14 weeks gestation in the right adnexa. The patient
presented with lower abdominal pain. This abdominal ectopic pregnancy was treated with direct
injection of potassium chloride and methotrexate into the gestational sac under transvaginal
ultrasound guidance. No further intervention was needed and the woman’s symptoms improved
immediately following this procedure.
Trường hợp hiếm gặp của TNTC là thai trong ổ bụng. Thai càng lớn thì bệnh suất của mẹ càng
cao. Bánh nhau bám vào ruột hoặc mạch máu chậu có thể gây chảy máu đáng kể nếu cố gắng
bóc nhau. Nếu gặp trường hợp thai trong ổ bụng giai đoạn lớn, lấy thai nhi một cách thận trọng
và giữ lại bánh nhau để tránh mất máu nhiều. Hình 13.25 và 13.26 minh họa 1 trường hợp thai
trong ổ bụng khoảng 14 tuần ở vùng chậu phải. Bệnh nhân có triệu chứng đau bụng dưới. Khối
thai trong ổ bụng này được điều trị bằng tiêm trực tiếp potassium chloride và methotrexate vào
túi thai dưới hướng dẫn của siêu âm. Triệu chứng của thai phụ được cải thiện ngay lập tức sau
khi làm thủ thuật này.
cao. Bánh nhau bám vào ruột hoặc mạch máu chậu có thể gây chảy máu đáng kể nếu cố gắng
bóc nhau. Nếu gặp trường hợp thai trong ổ bụng giai đoạn lớn, lấy thai nhi một cách thận trọng
và giữ lại bánh nhau để tránh mất máu nhiều. Hình 13.25 và 13.26 minh họa 1 trường hợp thai
trong ổ bụng khoảng 14 tuần ở vùng chậu phải. Bệnh nhân có triệu chứng đau bụng dưới. Khối
thai trong ổ bụng này được điều trị bằng tiêm trực tiếp potassium chloride và methotrexate vào
túi thai dưới hướng dẫn của siêu âm. Triệu chứng của thai phụ được cải thiện ngay lập tức sau
khi làm thủ thuật này.

Figure 13.25 A and B: Transvaginal ultrasound of an abdominal ectopic pregnancy at 14
weeks gestation in the right pelvis. Figure 13.25-A shows a sagittal view of the uterus with
pelvic free fluid (asterisks). Figure 13.25-B shows the abdominal pregnancy (arrows) in the
right pelvis.
Hình 13.25 A và B: Siêu âm qua ngả âm đạo thai trong ổ bụng khoảng 14 tuần ở vùng chậu
phải. Hình A với mặt cắt dọc tử cung cho thấy dịch tự do ở vùng chậu. Hình B: thai trong ổ
bụng ở vùng chậu phải
phải. Hình A với mặt cắt dọc tử cung cho thấy dịch tự do ở vùng chậu. Hình B: thai trong ổ
bụng ở vùng chậu phải

Figure 13.26: Transvaginal ultrasound of an abdominal ectopic pregnancy at 14 weeks
gestation in the right pelvis (same as in figure 13.25) following direct injection of potassium
chloride and methotrexate. The uterus (labeled) is seen separate from the ectopic pregnancy.
The macerated fetal head is labeled.
Hình 13.26: Siêu âm qua ngả âm đạo thai trong ổ bụng khoảng 14 tuần ở vùng chậu phải
(cùng bệnh nhân ở hình 13.25) sau khi tiêm potassium chloride và methotrexate. Tử cung
nằm tách biệt với khối thai. Mũi tên chỉ đầu thai nhi đã chết lưu.
(cùng bệnh nhân ở hình 13.25) sau khi tiêm potassium chloride và methotrexate. Tử cung
nằm tách biệt với khối thai. Mũi tên chỉ đầu thai nhi đã chết lưu.
CLIP 13.1

References:
1) Nederlof KP, Lawson HW, Saftlas AF, Atrash HK, Finch EL. Ectopic pregnancy
surveillance, United States, 1970–1987. In: CDC Surveillance Summaries. MMWR
1990; 39(no. SS-4):9–17.
2) Ectopic pregnancy – United States, 1990-1992.MMWR Morb Mortal Wkly Rep 44:46,
1995.
3) Goyaux N, Leke R, Keita N, Thonneau P. Ectopic pregnancy in African developing
countries. Acta Obstet Gynecol Scand 2003; 82(4):305-12.
4) Pisarka M, Carson SA, Buster JE. Ectopic pregnancy. Lancet 1998;351:1115
5) Breen JL. A 21 year survey of 654 ectopic pregnancies. Am J Obstet Gynecol
1970;106:1004
6) Schwartz RO, Di Pietro DL. Beta-HCG as a diagnostic aid for suspected ectopic
pregnancy. Obstet Gynecol 1980; 56:197.
7) Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta
accreta and cesarean scar pregnancy. A review. Timor-Tritsch IE, Monteagudo A. Am J
Obstet Gynecol. 2012 Jul;207(1):14-29
8) The diagnosis, treatment, and follow-up of cesarean scar pregnancy. Timor-Tritsch IE,
Monteagudo A, Santos R, Tsymbal T, Pineda G, Arslan AA. Am J Obstet Gynecol. 2012
Jul;207(1):44.e1-13
9) Discriminatory HCG zone; its use in the sonographic evaluation of ectopic pregnancy.
Kadar N, DeVore G, Romero R. Obstet Gynecol 1981; 58:156-161.
Nhận xét
Đăng nhận xét