Ultrasound in the Second Trimester
INTRODUCTION
The main objective of a second trimester ultrasound examination is to accurately date the
pregnancy, evaluate fetal anatomy, and assess placental location and the adnexae. Second
trimester components of the basic ultrasound examination are listed in Table 5.1 and may vary
based upon the level of support provided by the local health care system and national guidelines.
Mục tiêu chính của siêu âm tam cá nguyệt thứ hai là xác định lại chính xác tuổi thai,
khảo sát hình thái học thai nhi, vị trí bánh nhau và khảo sát hai phần phụ. Các bước cơ
bản cần được khảo sát trong tam cá nguyệt giữa được liệt kê trong bảng 5.1 và có thể
thay đổi tùy theo điều kiện hiện có của hệ thống y tế từng vùng và phác đồ của mỗi
quốc gia.
TABLE 5.1
Components of the Basic Second Trimester
Ultrasound Examination
- Fetal presentation and position
- Cardiac activity
- Fetal number (and chorionicity if multiple pregnancy)
- Fetal age/size (biometry)
- Amniotic fluid assessment
- Placental appearance and location
- Basic fetal anatomy
- Assessment of the adnexae
Bảng 5.1
Các bước khảo sát cơ bản trong siêu âm tam
cá nguyệt thứ hai
- Ngôi thai và vị trí thai
- Hoạt động của tim thai
- Số lượng thai ( và số bánh nhau nếu trong đa thai)
- Tuổi thai/ kích thước ( các chỉ số sinh học của thai)
- Lượng ối
- Hình thái và vị trí bánh nhau
- Cấu trúc giải phẫu cơ bản của thai
- Đánh giá phần phụ
TIMING OF THE SECOND TRIMESTER ULTRASOUND EXAMINATION
It is generally accepted that the “second trimester/mid-trimester” refers to the period of 14-28
weeks of gestation, but for the sake of this chapter, we are referring to the second trimester as an
ultrasound performed within the gestational period of 18 – 22 weeks. In countries where access
to ultrasound clinics is difficult or limited, this time period can be extended to 16-25 weeks of
gestation, with same caveats. At 16 weeks, the basic anatomy survey is more challenging than
later in gestation, especially when portable ultrasound equipment is used and/or in obese women.
On the other hand, dating a pregnancy at 25 weeks or greater, in the absence of a previous
ultrasound, is much less precise than earlier in gestation.
Nhìn chung, siêu âm tam cá nguyệt thứ hai là nói đến thời điểm 14-28 tuần, nhưng
trong khuôn khổ của chương này, chúng tôi chỉ đề câp tới siêu âm giai đoạn từ 18- 22
tuần trong tam cá nguyệt thứ hai. Ở những quốc gia mà người dân không có điều kiện
thuận lợi để tiếp cận hệ thống chăm sóc y tế hay không đến được phòng khám siêu âm
thì mốc thời này có thể nới rộng từ 16- 25 tuần với các bước khảo sát tương tự. Ở tuần
thứ 16, khảo sát hình thái thai nhi khó hơn những tuần sau đó, đặc biệt khi sử dụng
máy siêu âm cầm tay hoặc những phụ nữ béo phì. Mặt khác, nếu không có siêu âm
trước, việc xác định tuổi thai từ tuần 25 trở đi sẽ kém chính xác.
Who should perform the ultrasound examination?
The operator performing the ultrasound examination differs according to local rules and
traditions. In some countries, sonographers do the ultrasound examination and doctors review
them; in other countries, doctors primarily do the ultrasound examinations. In certain locations,
midwives perform the basic ultrasound examinations, whereas the doctors perform the targeted
ultrasound examinations. This last approach is most applicable to low-resource (outreach)
countries, due to shortage of medical personnel.
Tùy theo từng quy định và phong tục của từng địa phương, người siêu âm có thể là
những đối tượng khác nhau. Ở một vài quốc gia, kĩ thuật viên sẽ thực hành siêu âm và
sau đó bác sĩ sẽ xem lại. Ở một số quốc gia khác, bác sĩ sẽ là người siêu âm đầu tiên.
Ở một số ít nơi, nữ hộ sinh thực hiện những siêu âm cơ bản, còn bác sĩ sẽ siêu âm
khảo sát ở những mốc quan trọng và các trường hợp đặc biệt. Cách tiếp cận cuối phù
hợp với những quốc gia hạn chế về nguồn lực, thiếu nhân viên y tế.
Based upon our experience in low-resource
settings, where sonographers are typically not available and healthcare workers are in short
demand, midwives, when trained appropriately in didactic and hands-on supervised courses with
competency evaluation, can achieve a basic ultrasound skill that allows for limited ultrasound
examinations. Irrespective of the model in place, it is critical to ensure that operators performing
the ultrasound examinations are skilled and trained in the performance of these examinations.
Dựa vào kinh
nghiệm của chúng tôi, ở những nơi thiếu nguồn nhân lực, không có kĩ thuật viên siêu
âm hay nhân viên y tế không đáp ứng đủ cho nhu cầu người dân, cần tổ chức những
khóa huấn luyên bài bản về lí thuyết cũng như thực hành cho nữ hộ sinh với sự giám
sát và lượng giá để họ có kĩ năng cơ bản đủ để thực hiên một số loại siêu âm cơ bản.
Bất kể hình thức nào thì người thực hiện siêu âm khảo sát hình thái phải được đào tạo
và huấn luyện kỹ năng cần thiết.
In several countries, guidelines for the performance of the basic ultrasound examination and the
qualifications of the healthcare workers to perform such examinations are established. Readers
who wish to review these guidelines and qualifications are referred to the American Institute of
Ultrasound in Medicine (www.AIUM.org) and the International Society of Ultrasound in
Obstetrics and Gynecology (www.ISUOG.org) websites.
Ở nhiều nước, người ta đưa ra một phác đồ thống nhất cho những bước cơ bản thực
hiện và tiêu chuẩn lượng giá đối với người thực hiện những kĩ thuật siêu âm đó. Bạn
đọc có nhu cầu tham khảo hướng dẫn cụ thể và tiêu chuẩn lương giá có thể xem trên
trang website của hiệp hội siêu âm của Mỹ (www.AIUM.org) và tổ chức sản phụ khoa
quốc tế (www.ISUOG.org)
Preparation for the ultrasound examination
Before the ultrasound examination is initiated the operator should have a good understanding of
the physical principles of ultrasound, the basic operations of the ultrasound equipment and basic
technical skills for the performance of the ultrasound examination, details of which are provided
in Chapters 1, 2 and 3. Table 5.2 provides an itemized list that needs to be checked before the
initiation of any obstetric mid-trimester ultrasound examination.
Trước khi thực hiện siêu âm, người thực hiện cần hiểu rõ nguyên lí siêu âm, cách vận
hành cơ bản của máy, các kĩ thuật cơ bản, tất cả đã được mô tả chi tiết trong chương
1, 2 và 3. Bảng 5.2 mô tả danh sách những bước cần được kiểm tra trước khi thực
hiện bất kì quá trình siêu âm nào trong tam cá nguyệt thứ 2.
Table 5.2
Itemized List to be Checked Before Initiation of the Second
Trimester Ultrasound
- Ensure that the woman’s position on the ultrasound bed is comfortable
- Choose the obstetric setting on ultrasound machine
- Enter the woman’s name and other identifiers
- Enter the woman’s last menstrual period
- Place gel on the abdomen
- Adjust the gain settings
- Adjust the depth and focal ranges
- Use the correct orientation of the transducer when scanning
Bảng 5.2
Danh sách các bước cần được kiểm tra trước khi thực
hiện siêu âm trong 3 tháng giữa.
- Cần cho sản phụ nằm đúng tư thế, giường nằm trong quá trình được
siêu âm phải thoải mái.
- Chọn chế độ cài đặt sản khoa cho máy siêu âm
- Điền tên và những thông tin khác của sản phụ vào máy
- Điền kinh cuối
- Bôi gel lên bụng bệnh nhân
- Chỉnh gain sáng tối phù hợp
- Chỉnh độ sâu và vùng tập trung của sóng siêu âm
- Định hướng đầu dò đúng khi siêu âm.
When performing an obstetric ultrasound examination in low-resource settings, the second
trimester ultrasound examination can be simplified to six standardized steps, which are geared
towards the identification of findings that have a direct impact on the wellbeing of the mother
and fetus. These six steps are designed to assess fetal presentation and lie, the presence of fetal
cardiac activity, the number of fetuses within the uterus, the adequacy of the amniotic fluid, the
localization of the placenta and pregnancy dating. The technical aspects of five of these six steps
are described and illustrated in Chapter 10. We will hereby describe the sixth step, which
involves the biometric measurement of the fetus, including the biparietal diameter, the head
circumference, the abdominal circumference and the femur length.
Trong trường hợp thiếu nhân lực, siêu âm 3 tháng giữa cần được đơn giản hóa thành 6
bước chuẩn, nhằm tìm kiếm những vấn đề chính có ảnh hưởng trực tiếp đến mẹ và
thai nhi. 6 bước này được lập ra nhằm đánh giá ngôi thai, tư thế, hoạt động tim thai, số
lượng thai trong tử cung, lượng nước ối, vị trí bánh nhau, và tuổi thai. Ở đây, chúng ta
sẽ mô tả bước thứ 6, liên quan đến các chỉ số sinh học của thai, trong đó gồm đường
kính lưỡng đỉnh, chu vi đầu, chu vi bụng, và chiều dài xương đùi.
Fetal Biometry
Fetal biometry refers to fetal age and corresponds to the length of gestation (dating) while size
refers to the fetal weight and will be discussed later. Caution! A pregnancy should not be redated if a prior appropriate ultrasound examination established pregnancy dates. Re-dating on the
basis of 2nd trimester biometry should only be performed if the woman has not undergone any
other earlier ultrasound in pregnancy in which dating was established. Although ultrasound
dating in pregnancy is accurate in the second trimester, it is less precise than in the first trimester
of pregnancy, when pregnancy is dated by crown-rump length measurement.
Chỉ số sinh học có liên quan với tuổi thai và thời gian mang thai, trong khi đó, kích
thước liên quan đến cân nặng và sẽ được bàn luận sau. Lưu ý: không nên xác định lại
tuổi thai khi đã có tuổi thai theo siêu âm trước đó. Trong trường hợp thai phụ chưa có
siêu âm lần nào trước đó, có thể tính tuổi thai dựa vào các chỉ số sinh học trong tam cá
nguyệt thứ 2. Mặc dù việc tính tuổi thai có thể dựa trên siêu âm trong ba tháng giữa
nhưng mức độ chính xác thấp hơn so với siêu âm ba tháng đầu, dựa trên chiều dài đầu
mông.
We recommend the
following parameters for pregnancy dating in the second trimester:
- For pregnancies between 14 0/7 weeks and 15 6/7 weeks gestation, a discrepancy of more
than 7 days should result in a change in the Expected Date of Delivery (EDD).
- For pregnancies between 16 0/7 weeks and 21 6/7 weeks gestation, a discrepancy of more
than 10 days should result in a change in the EDD.
- For pregnancies between 22 0/7 weeks and 27 6/7 weeks gestation, a discrepancy of more
than 14 days should result in a change in the EDD.
Chúng tôi khuyến cáo nên tính tuổi thai theo các chỉ số trong tam cá nguyệt giữa
trong các trường hợp sau:
- Đối với thai từ 14 tuần đến 15 tuần 6 ngày, nếu có sự chênh lệch tuổi thai hơn 7
ngày cần tính lại ngày dự sinh.
- Đối với thai kì từ 16 tuần đến 21 tuần 6 ngày, nếu có sự chênh lệch hơn 10 ngày
nên tính lại ngày dự sinh
- Đối với thai kì từ 22 tuần đến 27 tuần 6 ngày, nếu có sự chênh lệch hơn 14 ngày
nên tính lại ngày dự sinh
Four fetal biometric measurements are required for dating and/or for estimating fetal weight
including the Biparietal Diameter (BPD), the Head Circumference (HC), the Abdominal
Circumference (AC) and the Femur Length (FL). In the following sections, measurement of each
of these 4 biometric parameters is explained in details.
Bốn chỉ số sinh học dùng để tính tuổi thai hoặc ước lượng cân nặng gồm đường kính
lưỡng đỉnh (ĐKLĐ), chu vi đầu (CVĐ), chu vi bụng (CVB), chiều dài xương đùi (CDXĐ).
Cách đo 4 chỉ số này sẽ được giải thích chi tiết trong những phần sau.
Biparietal Diameter
The Biparietal Diameter (BPD) (Figures 5.1 and 5.2) should be measured in a cross-sectional
view of the fetal head at the level of the thalami. Sonographic landmarks identifying the correct
BPD plane are listed in Table 5.3 and the procedure to measure the BPD is shown in Table 5.4.
On occasions, especially in the third trimester when the fetal head is engaged, the BPD can be
measured from a coronal plane of the head, if this is the only imaging option available.
Đường kính lưỡng đỉnh (ĐKLĐ) (Bảng 5.1 và 5.2) nên được đo theo mặt cắt ngang của
đầu ở ngang mặt cắt đồi thị. Các điểm mốc trên siêu âm của một mặt cắt lưỡng đỉnh
chuẩn được liệt kê theo Bảng 5.3 và cách thực hiện được liệt kê trong bảng 5.4. Trong
vài trường hợp, đặc biệt trong 3 tháng cuối, đầu xuống, ĐKLĐ được đo ở mặt phẳng
trán của đầu, nếu đây là lựa chọn duy nhất có thể
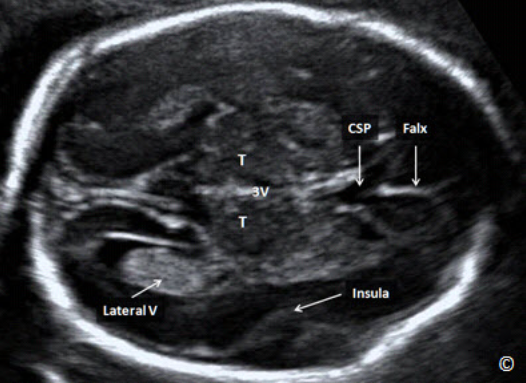
Figure 5.1: A transverse plane of the fetal head at the level of the biparietal diameter (BPD). In this
plane, you should see the cavum septae pellucidi (CSP), the falx (labeled), the thalami (T), 3rd
ventricle (3V) and the insula (labeled). A portion of the lateral ventricle is also seen (labeled).
Hình 5.1: Mặt cắt ngang của đầu ở đường kính lưỡng đỉnh. Ở mặt cắt này cho thấy vách trong suốt
(CSP), liềm não (Falx), đồi thị (T), não thất ba (3V), thùy đảo (insula) Một phần của não thất bên cũng
đươc ghi nhận ở mặt cắt này (Lateral V).

Figure 5.2: Transverse plane of the fetal head at the level of the biparietal diameter (BPD) showing
correct caliper placement. Note that the upper and lower calipers are traditionally placed on the
outer and inner edge(s) of the cranium respectively (GA = gestational age and EFW = estimated fetal
weight).
Hình 5.2: Mặt cắt ngang lưỡng đỉnh cho thấy vị trí đúng khi đặt con trỏ để đo. Chú ý điểm trên và dưới
của điểm đo là bờ ngoài bản sọ gần và bờ trong của bản sọ xa. (GA = gestational age- tuổi thai và EFW
= estimated fetal weight- ước lượng cân nặng).
Sonographic Landmarks for the Measurement of the Biparietal
Diameter Plane (BPD). See Figure 5.1
- Midline Falx
- Thalami
- Symmetrical appearance of both cerebral hemispheres
- No cerebellum visualized
- Cavum Septae Pellucidi
- Insula
Mốc giải phẫu trên siêu âm ở mặt cắt đo đường kính
lưỡng đỉnh. Xem hình minh họa 5.1
- Liềm não ở đường giữa
- Đồi thị
- Sự hiện diện cân xứng cấu trúc 2 bán cầu não
- Không thấy tiểu não
- Vách trong suốt
- Thùy đảo
Table 5.
Procedure for the Measurement of the Biparietal Diameter (BPD).
See Figure 5.2
- Activate the biometry software (calculate knob) on the console of the ultrasound
equipment
- Select the BPD option, a caliper will appear on the monitor
- Position the caliper on the outer edge of the proximal parietal bone, roughly at the
level of the thalami, where the head is wider, and set it
- Position the second caliper, symmetrically, on the inner edge of the distal parietal
bone, in such a way that the line between the two calipers is at 90° with the
midline falx, and set it.
- Ensure that the BPD measurement is the widest possible and is perpendicular to
the midline falx.
Tiến trình đo đường kính lưỡng đỉnh (BPD)
Xem hình 5.2
- Vào mục đo các chỉ số sinh học (ấn vào nút đo trên bàn phím) trên máy siêu âm.
- Chọn BPD, thang đo sẽ xuất hiện trên màn hình.
- Vị trí của thanh đo thứ 1 đặt ở bờ ngoài bản sọ đính gần, ngang mức đồi thị.
- Đặt con trỏ thanh đo thứ 2 ở bờ trong bản sọ xa, chú ý đường nối 2 điểm đó vuông
góc với đường giữa liềm não.
- Đảm bảo sao cho đường kính lưỡng đỉnh là lớn nhất và vuông góc với đường giữa
liềm não.
Head Circumference
The Head Circumference (HC) is measured in the trans-thalamic view, which is the same plane
as that for the BPD measurement (Figure 5.1 and 5.2). There are three options for the
measurement of the HC on most ultrasound equipment; the ellipse method (Figure 5.3), the 2-
diameter method and the trace method. The ellipse method allows the operator to expand an
ellipse over the cranium, typically by initially fixing the BPD and occipito-frontal diameters
(OFD). The 2-diameter method utilizes the 2 diameters (BPD and OFD) and calculates the HC
from an ellipsoid formula. The tracing method simply traces the cranium as seen on the display
monitor.
Chu vi đầu (CVĐ) được đo ở mặt cắt ngang đồi thị, cùng mặt cắt đo lưỡng đỉnh (hình
5.1 và 5.2). Có 3 cách đo chu vi vòng đầu trên hầu hết các máy siêu âm: đo bằng vòng
ellipse (hình 5.3), đo 2 đường kính và đo bằng cách vẽ tay xung quanh chu vi đầu.
Cách đo bằng ellipse cho phép điều chỉnh kích thước vòng tròn ellipse quanh hộp sọ,
thường ta sẽ đặt điểm đo cố định trước ở 2 đường kính lưỡng đỉnh và đường kính đỉnh
chẩm (ĐKĐC).Phương pháp đo 2 đường kính được sử dụng dựa vào 2 đường kính (ĐKLĐ và ĐKĐC) và tính ra chu vi đầu dựa vào công thức ellipse. Phương pháp đo bằng tay đơn giản là chỉ vẽ theo chu vi hộp sọ như hình trên màn hình hiển thị.
Of the three methods that can be selected on most ultrasound equipment, the ellipse
method is preferred as it has the least inherent error (Figure 5.3). The authors recommend that
you perform the HC measurement following the BPD measurement. This approach allows the
operator to utilize the calipers placed for BPD measurement, which expedites the process. It is of
note that when the HC is being measured, the lower caliper from the BPD diameter should be
moved to the outer bony parietal edge (Figure 5.4). Table 5.5 lists the steps for the measurement
of the HC.
Trong 3 cách trên thì cách đo theo hình ellipse là hay được dùng nhất do nó vốn ít sai số. Tác
giả khuyến cáo bạn nên thực hiện đo CVĐ theo đường kính lưỡng đỉnh. Cách tiếp cận
này cho phép máy sử dụng thanh đo của đường kính lưỡng đỉnh. Chú ý rằng trong quá
trình đo CVĐ, điểm đo dưới của ĐKLĐ cần di chuyển sang bờ ngoài của bản sọ đính
để đo CVĐ. (hình 5.4). Bảng 5.5 nêu ra những bước cần cho đo chu vi đầu.

Figure 5.3: Transverse plane of the fetal head at the biparietal diameter (BPD) level. The head
circumference (HC) is measured using the ellipse method. Note that the ellipse is tracing the outer
edge of the fetal cranium. (OFD= occipito-frontal diameter, GA=gestational age, EFW=estimated fetal
weight, CI=cephalic index and FL = femur length).
Hình 5.3: Mặt cắt ngang đầu ở vị trí để đo lưỡng đỉnh. Chu vi đầu (CVĐ) được đo bằng phương pháp
ellipse. Chú ý vòng ellipse bao quanh bờ ngoài bản sọ. (OFD= occipito-frontal diameter: Đường kính
chẩm-trán, GA=gestational age: tuổi thai, EFW=estimated fetal weight: cân nặng, CI=cephalic index:

Figure 5.4: Transverse plane of the fetal head at the biparietal diameter (BPD) level. The head
circumference (HC) is measured using the ellipse method. Note that the ellipse is tracing the outer
edge of the fetal cranium, and the lower caliper for BPD measurement is placed at the inner edge of
the parietal bone. (OFD= occipito-frontal diameter, GA=gestational age and CI=cephalic index).
Hình 5.4: mặt cắt ngang ở vị trí đo đường kính lưỡng đỉnh (ĐKLĐ). Chu vi đầu được đo bằng vòng
ellipse. Chú ý: vòng ellipse bao ở bờ ngoài của bản sọ, con trỏ phía dưới đo ĐKLĐ nằm ở bờ trong bản
sọ.
TABLE 5.5 Procedures for the Measurement of the Head Circumference
- Activate the biometry software (Calculate knob) on the scanner console, select the HC and a
caliper will appear on the screen
- Position the caliper on the outer edge of the proximal parietal bone, similar to the BPD
measurement, and set it
- Position the second caliper, symmetrically, on the outer edge of the distal parietal bone, in
such a way that the line between the two calipers is at 90° with the midline falx, and set it
- Open up the ellipse by rotating the trackball on the console sideways, until the ellipse is
perfectly overlaid on the skull contour
- If the ellipse is not aligned with the ovoid of the fetal head, change the position of the two
calipers, which act as hinges
Bảng 5.5 Tiến trình đo chu vi vòng đầu
- Kích hoạt phần mềm đo các chỉ số sinh học (nhấn vào nút đo) trên bàn điều khiển
máy siêu âm, chọn HC, con trỏ thanh đo sẽ xuất hiện trên màn hình.
- Đặt con trỏ thứ nhất của thanh đo ở bờ ngoài bản sọ đính gần, tương tự như đo
ĐKLĐ và nhấn phím SET.
- Đặt con trỏ thứ hai của thanh đo, đối xứng qua đường giữa, ở bờ ngoài của bản sọ
xa, và nhấn SET, trong trường hợp này, đường nối 2 điểm đo vuông góc với liềm não
ở đường giữa.
- Mở vòng ellipse rộng ra bằng cách xoay thanh lăn trên bàn phím điều khiển, cho đến
khi vòng ellipse viền quanh ôm lấy bờ cong hộp sọ.
- Nếu vòng ellipse không viền quanh được hình ovale của đầu, thì ta cần chỉnh lại vị trí
đặt của 2 con trỏ vì nó chính là trục để xoay của vòng đo ellipse.
Abdominal Circumference
The Abdominal Circumference (AC) is measured on a transverse section of the upper fetal
abdomen. Sonographic landmarks identifying the correct plane for the AC measurement are
listed in Table 5.6 and Figure 5.5.
Chu vi bụng (CVB) được đo ở mặt cắt ngang bụng trên của thai nhi. Các mốc giải phẫu
trên siêu âm giúp xác định mặt cắt chuẩn đo chu vi bụng được liệt kê ở Bảng 5.6 và
hình 5.5.
TABLE 5.6 Sonographic Landmarks for the Abdominal Circumference (AC)
- Circular cross section of the abdomen (as circular as possible)
- Spine seen on cross section
- Stomach bubble
- Intra-hepatic portion of the umbilical vein at the level of the portal sinus
- Large sections of fetal ribs seen on each side laterally
- Kidneys not be visualized in the image
BẢNG 5.6 Các mốc giải phẫu trên siêu âm cho mặt cắt đo chu vi bụng:
- Mặt cắt ngang bụng phải tròn ( càng tròn càng tốt)
- Xương cột sống phải được quan sát ở mặt cắt ngang.
- Bóng hơi dạ dày.
- Tĩnh mạch rốn đoạn trong gan ở ngang mức xoang tĩnh mạch cửa
- Phần lớn cung xương sườn được quan sát thấy ở 2 bên.
- Không thấy thận ở mặt cắt này
Care should be taken to ensure that the cross-section of the abdomen is as circular as possible, in
order to avoid errors in the measurement. This is easier in the 2nd than the 3rd trimester, when the
fetal limbs or shadowing can indent the abdominal circumference (Figure 5.6). The AC is best
measured with the fetal spine at 3 or 9 o’clock (Figure 5.7 A and B). Avoid measuring the AC if
at all possible when the fetal spine is at 6 or 12 o’clock (Figures 5.6 and 5.8 A and B). The
procedure to measure the AC is shown in Table 5.7.
Nên chú ý mặt cắt ngang bụng phải càng tròn càng tốt, tránh những sai số do đo đạc.
Việc này dễ thực hiện ở tam cá nguyệt thứ 2 hơn ở tam cá nguyệt thứ 3, do tay chân
hoặc bóng lưng có thể che lấp hình ảnh chu vi bụng chuẩn. (hình minh họa 5.6). Mặt
cắt chu vi bụng tốt nhất được đo khi cột sống nằm ở vị trí 3 hoặc 9 giờ (xem hình 5.7 A
và B). Tránh đo chu vị bụng khi cột sống nằm ở vị trí 6 hoặc 12 giờ (hình 5.6, 5.8 A và
B). Các bước đo chu vi bụng được liệt kê trong Bảng 5.7.

Figure 5.5: Transverse plane of the fetal abdomen at the anatomic level of the abdominal
circumference. Note the anatomic landmarks that include the stomach bubble (St), the umbilical vein
(UV), the descending aorta (Ao) and the inferior vena cava (IVC). The spine (S) is seen at 3 o’clock and
one full rib (Rib) on each side.
Hình 5.5: Mặt cắt ngang bụng chuẩn với các mốc giải phẫu như trên hình dùng để đo chu vi bụng. Chú
ý: bóng hơi dạ dày (st), tĩnh mạch rốn (UV), động mạch chủ xuống (Ao) và tĩnh mạch chủ dưới (IVC),
quan sát thấy cột sống (S) ở vị trí 3 giờ và toàn bộ cung sườn 2 bên. (Rib)

Figure 5.6: Transverse plane of the fetal abdomen at the level of the abdominal
circumference (AC) in the third trimester of pregnancy. Note the shadowing (arrows) from
upper extremity bones, obscuring the AC lateral borders. The spine (S) is at the 12 o’clock
position, which makes optimal measurement of AC difficult.
Hình 5.6: Mặt cắt ngang bụng đo chu vi bụng trong 3 tháng cuối. Chú ý hình ảnh bóng lưng (mũi tên
chỉ) do xương chi trên tạo ra làm mờ đường giới hạn của chu vi bụng ở 2 bên. Cột sống (S) ở vị trí 12
giờ, sẽ hạn chế việc đo chu vi bụng chính xác.

Figure 5.7 A and B: Transverse planes of the fetal abdomen at the level of the abdominal
circumference (AC). The spine (S) is at the 9 o’clock position in A and at the 3 o’clock position in B.
Spine positions at 9 or 3 o’clock are most optimal for AC measurement as it minimizes shadowing.
Hình 5.7 A và B: minh họa mặt cắt ngang để đo chu vi bụng (AC). Cột sống (S) ở vị trí 9 g, ở hình A
và 3 g ở hình B. Cột sống ở vị trí 9 hoặc 3 g thường sẽ dễ đo được chu vi bụng chính xác nhất, do nó
ít bị bóng lưng che khuất.
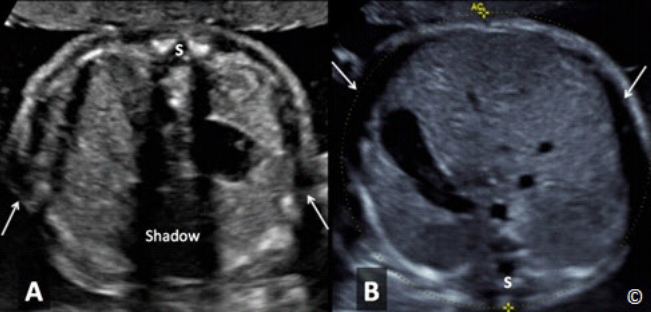
Figure 5.8 A and B: Transverse planes of the fetal abdomen at the level of the abdominal
circumference (AC). The spine (S) is at the 12 o’clock position in A and at the 6 o’clock position in B.
Spine position at 12 or 6 o’clock is the least optimal for AC measurement as it increases shadowing
(A-labeled) and minimizes the ability to assess the lateral borders (arrows) (A and B) due to
decrease in lateral resolution and rib shadowing.
Hình 5.8 A và B: minh họa mặt cắt ngang chu vi bụng. Cột sống (S) ở vị trí 12g ở hình A và 6g ở hình
B. Cột sống ở vị trí 12g hay 6g là mặt cắt kém chính xác nhất trong việc đo chu vi bụng do nó tăng
bóng lưng (hình A) và giảm khả năng đánh giá giới hạn bên (mũi tên) (hình A và B) do nó giảm độ
phân giải ngang của tia siêu âm và có bóng lưng xương sườn.
TABLE 5.7 Procedures for the Measurement of the Abdominal Circumference (AC)
- Activate the biometry software on the scanner console (Calculate knob), select the
AC and a caliper will appear on the screen
- Position the caliper on the outer surface of the skin line, on the proximal side of the
fetal abdomen, roughly at the level of the rib end, and set it
- Position the second caliper, symmetrically, on the distal surface of the skin line, in
such a way that the line between the two calipers is at 90° with the midline, and set
it
- Open up the ellipse by rotating the trackball on the console sideways, until the
ellipse is perfectly overlaid on the skin contour. Ensure to include the outer edge of
the skin contour with the measurement
- If the ellipse is not aligned with the cutaneous outline of the abdomen, change the
position of the two calipers, which act as hinges
BẢNG 5.7 Các bước thực hiện đo chu vi bụng (CVB)
- Kích hoạt phần mềm đo các chỉ số sinh học (nhấn vào nút đo) trên bàn điều
khiển máy siêu âm, chọn AC, con trỏ thanh đo sẽ xuất hiện trên màn hình.
- Cố định 1 con trỏ đo ở bờ ngoài mặt da của bụng, phía bên bụng gần đầu
dò, gần điểm kết thúc cung sườn và nhấn nút SET để đo.
- Đặt con trỏ thứ 2 ở bờ ngoài da phía bên kia, đối xứng, tạo thành 1 đường
vuông góc với đường giữa, và nhấn nút SET.
- Mở vòng tròn ellipse bằng cách xoay con lăn phía bên bàn phím, cho tới khi
vòng ellipse bao trọn bờ ngoài da bụng.
- Nếu vòng ellipse không viền quanh đượ bờ ngoài da bụng, thì ta cần chỉnh
lại trí đặt của 2 con trỏ vì nó chính là trục để xoay của vòng ellipse.
Femur Length
In order to optimize the measurement of the Femur Length (FL), the whole femur diaphysis
should be displayed on the screen, and the angle between the insonating beam and the shaft of
the femur should be kept in the range of 45-90° in order to avoid underestimating the length of
the femur due to ultrasound wave deflection (Figure 5.9). The longest visible diaphysis should
be measured by placing each caliper at the end of the ossified diaphysis without including the
distal femoral epiphysis, if visible (Figure 5.10). Femur measurement should exclude triangular
spur artefacts that can falsely extend the diaphysis length (Figure 5.10).
Để đo chiều dài xương đùi chính xác nhất, cần nhìn thấy được toàn bộ thân xương, góc
tia siêu âm và thân xương đùi cần nằm trong khoảng 45-90 độ để tránh trường hợp đo
chiều dài xương đùi không chính xác do sóng siêu âm bị lệch hướng (hình 5.9). Chiều
dài thân xương dài nhất là khi con trỏ đo đặt ở 2 điểm cuối của phần thân xương được
cốt hóa mà không bao gồm mấu chuyển xa xương đùi (nếu thấy được) (hình 5.10). Đo
xương đùi cần loại trừ ảnh giả do gai xương có thể làm tăng giả chiều dài thân xương
đùi (hình5.10).

Figure 5.9: Optimal imaging of the femur for length measurement. Note that the
whole femur diaphysis is seen and the angle between the insonating beam (arrow)
and the shaft of the femur is almost 90 degrees.
Hình 5.9: hình minh họa mặt cắt đo xương đùi chuẩn nhất. Chú ý là toàn bộ thân xương đùi
được quan sát thấy và góc giữa tia siêu âm (hướng mũi tên) và trục xương đùi gần như 90 độ.

Figure 5.10: Femur length measurement. Note that the longest visible
diaphysis is measured by placing each caliper at the end of the ossified
diaphysis without including the distal femoral epiphysis (labeled).
Hình 5.10: cách đo chiều dài xương đùi. Chú ý xương đùi dài nhất có thể đo được khi ta đặt 2 con
trỏ đo ở đầu tận cùng của thân xương được cốt hóa và chừa mấu chuyển xa xương đùi (mũi tên)
It is important to note that imaging of the long axis of the femur can be more technically difficult
than the BPD, HC and AC. Consideration should therefore be given to delay the introduction of
the FL to the basic ultrasound examination, until more technical expertise is acquired by novice
ultrasound operators. If this course is chosen, formula for EFW that does not utilize FL should be
activated in the ultrasound equipment.
Cần lưu ý là kỹ thuật đo chiều dài của xương đùi sẽ khó hơn đo ĐKLĐ, CVĐ, và CVB.
Do đó, cần đặt ra việc trì hoãn đưa chiều dài xương đùi vào quy trình siêu âm cơ bản,
cho đến khi những người mới thực hành có kĩ năng siêu âm thuần thục hơn. Nếu sử
dụng quy trình này, không nên dùng chiều dài xương đùi để tính cân nặng thai.
Estimating Fetal Weight
Once the four measurements described above have been calculated, the software of the
ultrasound equipment derives the estimated fetal weight (EFW), using a mathematical formula.
Hadlock et al is the formula that is most commonly used for EFW and was developed in the late
1980s (1). Calculating the EFW is more accurate in the second trimester than the third trimester
but EFW is clearly of lesser clinical relevance in the second trimester. In the 3rd trimester, EFW
is of crucial importance to detect fetal growth restriction or macrosomia. The estimation of
macrosomia is not very accurate and the error can exceed 10% (2). Detailed discussion on
estimation of fetal weight will be presented in the following chapter.
Một khi có được 4 số đo trên, phần mềm siêu âm sẽ tính ra cân nặng ước lượng dựa
vào phần mềm toán học. Công thức của Hadlock và cộng sự là công thức thường được
sử dụng nhất để tính cân nặng, được phát triển từ những năm 1980 (1). Tính cân nặng
trong tam cá nguyệt thứ 2 chính xác hơn tam cá nguyệt thứ 3 nhưng ứng dụng lâm
sàng lại ít hơn. Trong tam cá nguyệt thứ 3, việc ước lượng cân nặng thai nhi khá quan
trọng trong việc phát hiện thai chậm tăng trưởng hoặc thai to. Việc ước lượng thai to
không quá chính xác và sai số có thể vượt quá 10%(2). Vấn đề này sẽ được bàn luận
chi tiết trong chương sau.
Basic Fetal Anatomy
Although fetal anatomy is part of the basic ultrasound examination as defined by national and
international organizations (3, 4), in some low-resource (outreach) settings, the primary objective
of the second trimester ultrasound is to identify high-risk pregnancies at increased risk for
neonatal and maternal morbidity and mortality. To that end, review of basic fetal anatomy is
typically not part of the basic ultrasound examination in that setting. Basic fetal anatomy is
presented in this chapter for completeness sake and also as it is part of the basic ultrasound
examination in the second and third trimester in many countries. Placental appearance, its
location within the uterine cavity, amniotic fluid assessment and the adnexae are also part of the
basic ultrasound examination. They are covered in separate chapters later in the book. Table 5.8
shows a list of basic fetal anatomy for the second trimester ultrasound.
Mặt dù khảo sát hình thái thai nhi là phần cơ bản của quy trình siêu âm sản như định
nghĩa của các tổ chức trong và ngoài nước (3, 4), nhưng ở một số nơi thiếu nhân lực,
mục tiêu tiên quyết của siêu âm 3 tháng giữa là phát hiện những thai kì nguy cơ cao có
thể làm gia tăng nguy cơ mắc bệnh và tử vong sau sanh ở sản phụ và thai nhi. Do đó,
khảo sát hình thái cơ bản thai nhi thường không phải là quy trình siêu âm cơ bản của
nơi đó. Giải phẫu thai cơ bản được nêu ra trong chương này mang lại lợi ích toàn diện
và cũng là quy trình siêu âm cơ bản được sử dụng ở nhiều nước đối với siêu âm ở tam
cá nguyệt thứ 2 và thứ 3. Hình dạng bánh nhau, vị trí nhau trong buồng tử cung, đánh
giá lượng ối, phần phụ cũng là một phần của các bước siêu âm cơ bản. Tất cả được
nêu trong những chương riêng biệt sau của quyển sách này. Bảng 5.8 liệt kê các cấu
trúc giải phẫu cơ bản cần khảo sát trong siêu âm tam cá nguyệt thứ 2.
For more information on the practice guideline for the performance of the basic obstetric
ultrasound examination, visit the American Institute of Ultrasound in Medicine
(www.AIUM.org) and the International Society of Ultrasound in Obstetrics and Gynecology
(www.ISUOG.org) websites (3, 4).
Để biết thêm thông tin của hướng dẫn thực hành về siêu âm sản khoa cơ bản, vui lòng
tham khảo trên trang web của Viện siêu âm y khoa Mỹ (www.AIUM.org) và của tổ chức
quốc tế về siêu âm sản phụ khoa (www.ISUOG.org) (3, 4).
TABLE 5.8 List of Basic Fetal Anatomy in the Second Trimester of Pregnancy
- HEAD
o Lateral cerebral ventricles, Choroid plexus, Midline falx, Cavum septae
pellucidi, Cerebellum, Cistern magna; and Upper lip and philtrum.
- CHEST
o Heart; Four-chamber view, Left ventricular outflow tract, Right
ventricular outflow tract and Lung fields.
- ABDOMEN
o Stomach (presence, size, and situs), Kidneys, Urinary bladder, Umbilical
cord insertion into the fetal abdomen, and Umbilical cord vessel number.
- SKELETAL
o Cervical, Thoracic, Lumbar, and Sacral spine.
- Extremities
o Legs and Arms
- PLACENTA
- AMNIOTIC FLUID
- ADNEXAE
Bảng 5.8 Các bước khảo sát hình thái học cơ bản trong tam cá nguyệt thứ hai
- ĐẦU
o Não thất bên, đám rối mạng mạch, liềm não, vách trong suốt, tiểu
não, bể lớn hố sau; môi trên và rãnh mũi-môi (nhân trung).
- NGỰC
o Tim; Mặt cắt 4 buồng, buồng thoát thất trái, buồng thoát thất phải
và cấu trúc phổi.
- BỤNG
o Dạ dày (có hay không, kích thước, vị trí), thận, bàng quang, dây
rốn cắm vào thành bụng thai nhi, số lượng mạch máu trong cuống
rốn.
- HỆ XƯƠNG
o Cột sống cổ, ngực, lưng, và cùng cụt.
- TỨ CHI
o Tay và chân
- BÁNH NHAU
- DỊCH ỐI
- PHẦN PHỤ
Head anatomy
Three axial sonographic planes are needed to assess the head anatomy: the plane at the level of
the lateral ventricles (Figure 5.11), the plane at the level of the BPD (Figure 5.2), and the plane
at the level of the posterior fossa (Figure 5.12).
3 mặt cắt ngang trên siêu âm cần dùng để đánh giá giải phẫu học vùng đầu: mặt cắt
ngang não thất bên (hình 5.11), mặt cắt ngang đường kính lưỡng đỉnh (Hình 5.2), và
mặt cắt ngang hố sau (hình 5.12)

Figure 5.11: Transverse plane of the fetal head at the level of the lateral ventricles
(LV). Sonographic landmarks for LV measurement include the LV, the cavum septae
pellucidi and the midline falx (labeled). The LV is measured at the level of the atrium
(asterisks). CP = Choroid Plexus.
Hình 5.11: Mặt cắt ngang đầu ỏ vị trí ngang não thất bên 2 bên (LV). Các mốc giải phẫu
của mặt cắt bao gồm não thất bên, vách trong suốt và liềm não (Falx). Não thất bên được
đo ở ngã ba của não thất (dấu sao). CP = Choroid Plexus: đám rối mạng mạch.

Figure 5.12: Transverse plane of the fetal head at the level of the posterior fossa.
Sonographic landmarks include the cerebellum, cisterna magna and falx (labeled).
Hình 5.12: mặt cắt ngang hố sau. Các mốc trên siêu âm gồm tiểu não, bể lớn hố sau và liềm não
Plane at level of Lateral Ventricles
Mặt cắt ngang não thất bên
This represents an axial view of the fetal head, at the level of the lateral ventricles (Figure 5.11).
Sonographic landmarks identifying the correct anatomic plane include the lateral ventricles, the
cavum septae pellucidi and the midline falx (Figure 5.11). On this view, the width of the atrium
of the distal lateral ventricle should be measured (Figure 5.11). Visualization of the proximal
lateral ventricle is obscured by proximal parietal bone shadowing (Figure 5.11). The atrium of
the lateral ventricle should be measured at the level shown in Figure 5.11 and should be equal to
or <10.0 mm. anytime in gestation.
Phần này giới thiệu mặt cắt ngang vùng đầu thai nhi, ngang qua 2 não thất bên( hình
5.11). Điểm mốc giải phẫu ở mặt cắt chuẩn trên siêu âm bao gồm: não thất bên, vách
trong suốt, đường giữa liềm não (hình 5.11). Trên mặt cắt này, ta nên đo độ rộng ở vị
trí giao nhau của não thất (atrium of lateral ventricular) (chỗ giao nhau của 3 sừng trán,
chẩm và sừng thái dương hay còn gọi là ngã ba não thất hoặc ngã tư não thất tùy tài
liệu dịch) của não thất bên đối diện, phía xa đầu dò (hình 5.11) do não thất bên phía
gần đầu dò sẽ bị che khuất bởi bóng xương sọ gần đầu dò (hình 5.11). Não thất bên
nên được đo ở vị trí như Hình 5.11 và bình thường nhỏ hơn hoặc bằng 10 mm ở bất kì
tuổi thai nào.
Ventriculomegaly is defined by a lateral ventricular
measurement of greater than 10 mm and is the most common intracranial malformation (Figure
5.13) diagnosed prenatally. Ventriculomegaly is associated with many intracranial
malformations and with fetal aneuploidy and its finding should therefore result in a targeted
ultrasound examination of fetal anatomy and counselling for fetal aneuploidy testing.
Dãn não thất được định nghĩa khi đường kính não thất bên > 10 mm,
cũng bất thường hay gặp nhất trong các bất thường trong não (hình 5.13) được chẩn
đoán trước sanh. Dãn não thất thường kết hợp với nhiều bất thường não khác và đi
kèm lệch bội, vì vậy, nếu phát hiện dãn não thất cần có sự tầm soát toàn diện trên siêu
âm và tư vấn kiểm tra bất thường nhiễm sắc thể.
Holoprosencephaly, which results from failure of division of the prosencephalon during early
embryogenesis into two lateral ventricles, can also be detected in this plane (Figure 5.14 A and
B). Anencephaly (absence of brain tissue associated with absent calvarium) (Figure 5.15 A and
B) and encephalocele (Figure 5.16 A and B), (localized defect of cranium – neural tube defect),
can also be detected in this plane.
Não thất duy nhất
(holoprosencephaly) cũng có thể phát hiện trên mặt cắt này, nguyên nhân của
holoprosencephaly là do trong quá trình phân chia phôi thai giai đoạn sớm, não trước
không phân chia hoàn chỉnh (Hình 5.14 A và B). Thai vô não (không có nhu mô não
thường kết hợp với không có hợp sọ) (Hình 5.15 A và B) và thoát vị não (Hình 5.16 A
và B), (khiếm khuyết khu trú của hợp sọ – khiếm khuyết ống thần kinh), cũng có thể
được phát hiện ở mặt cắt này

Figure 5.13: Transverse plane of the fetal head at the level of the
lateral ventricles (LV) in a fetus with bilateral ventriculomegaly. Note
the enlarged lateral ventricles (LV) and compressed cerebral cortex (C)
and choroid plexus (CP).
Hình 5.13: Mặt cắt ngang não thất bên 2 bên (LV) ỏ thai nhi có dãn não
thất 2 bên. Chú ý: não thất dãn rộng (LV) và vỏ não bị chèn ép (C), đám
rối mạng mạch (CP).

Figure 5.14 A and B: Holoprosencephaly in 2 fetuses shown in a transverse plane (A) and coronal
plane (B) of the fetal head. A single ventricle is seen (asterisk) with fused thalami (T). Note a
hypoplastic cerebellum (Cereb) in A (not typically a feature of holoprosencephaly).
Hình 5.14 A và B: Não thất duy nhất ở 2 phôi thai quan sát ở mặt cắt ngang đầu (A) và mặt phẳng
trán (B). 1 não thất (dấu sao) với đồi thị hòa nhập (T). Chú ý tiểu não thiểu sản ở hình A (Cereb) (là
dấu hiệu không điển hình của não thất duy nhất.

Figure 5.15 A and B: Imaging of the fetal head in 2 fetuses with anencephaly (A and B). Note the
absence of fetal cranium and normal brain tissue.
Hình 5.15 A và B: Cấu trúc đầu của 2 thai vô não (A và B). Chú ý: không quan sát thấy hộp sọ và nhu
mô não bình thường

Figure 5.16 A and B: Transverse planes of the fetal head in 2 fetuses (A and B) with encephaloceles
(E). Note the location of the cranial defect (arrows), in the occipital aspect of the cranium, which is
the most common location for such defects. Brain tissue can be seen in both encephaloceles (E).
Hình 5.16 A và B: Mặt cắt ngang của đầu ở 2 thai (A và B) có thoát vị não (E). Chú ý vị trí khiếm
khuyết vòm sọ (mũi tên) ở vùng chẩm là vị trí thường gặp nhất cho bất thường này. Mô não trong
khối thoát vị có thể thấy trong cả 2 trường hợp (E).
Plane at level of Posterior Fossa
Mặt cắt ngang hố sau
The plane at the level of the posterior fossa, also known as the trans-cerebellar plane, is an axial
(or slightly oblique) view at the level of the posterior fossa (Figure 5.17). In this plane you can
see the cerebellum, the cisterna magna, and the 3rd and 4th ventricles (Figure 5.17). This plane is
easily obtained by angling the ultrasound transducer posteriorly about 45 degrees from the BPD
plane while avoiding shadowing from the cranial bone.
Mặt cắt ngang hố sau, có thể gọi là mặt cắt ngang não, là mặt cắt chếch nghiêng nhẹ
về phía hố sau (Hình 5.17). Trong mặt cắt này có thể thấy tiểu não, bể lớn hố sau, não
thất ba và não thất tư (Hình 5.17). Ta có thể dễ dàng cắt được mặt cắt này khi chếch
đầu dò về phía sau 45 độ từ mặt cắt lưỡng đỉnh đồng thời tránh bóng lưng xương sọ
The most common abnormalities
detected in this view represent the Dandy-Walker malformation (Figure 5.18), cerebellar vermis
dysgenesis (Figure 5.19) and the Chiari II malformation (Figure 5.20) (typical of spina bifida).
Occasionally, posterior, small occipital encephaloceles may only become evident in this
scanning plane. Spina bifida (with Chiari II malformation) (Figure 5.20, 5.21 A and B) requires
neonatal surgery both to cover the spinal defect and to shunt the commonly associated
obstructive ventriculomegaly.
Những bất thường thường gặp nhất phát hiện ở mặt cắt này nằm trong bất thường
Dandy-Walker (Hình 5.18), loạn sản thùy nhộng tiểu não (hình 5.19) và bất thường
Chiari (Hình 5.20) (thường là chẻ đôi đốt sống). Thông thường, thoát vị não vùng chẩm
nhỏ, phía sau, chỉ có thể quan sát rõ ở mặt cắt này. Chẻ đôi đốt sống (với bất thường
Chiari II) (Hình 5.20, 5.21 A và B) đòi hỏi mổ sau sanh để che lấp khiếm khuyết vùng
tủy sống và đặt shunt thông với hệ thống não thất bị tắc nghẽn.

Figure 5.17: Transcerebellar plane of the fetal head (transverse – oblique). The posterior
fossa contains the cerebellum and cisterna magna (labeled). The 4th and 3rd ventricles (4V
and 3V) are seen in this plane.
Hình 5.17: Mặt cắt ngang não (ngang - chếch nghiêng). Hố sau chứa tiểu não (cerebellum),
bể lớn (cisterna magna). Não thất tư (4V) và não thất ba (3V) cũng quan sát thấy ở mặt cắt
này

Figure 5.18: Transcerebellar plane of a fetus with Dandy Walker malformation (asterisk).
Note the absence of the cerebellum and enlargement of cisterna magna (CM). Note the
presence of a cystic hygroma (CH) in this fetus.
Hình 5.18: Mặt cắt ngang tiểu não ở thai có bất thường Dandy Walker (dấu sao). Chú ý:
không quan sát thấy tiểu não và hố sau dãn rộng (CM), nang bạch huyết vùng cổ (CH)

Figure 5.19: Transcerebellar plane of a fetus with cerebellar vermis
dysgenesis (asterisk). Note the absence of the cerebellar vermis (CV)
with enlargement of cisterna magna (asterisk).
Hình 5.19: mặt cắt ngang tiểu não ở thai có loạn sản thùy nhộng (dấu
sao). Chú ý: không quan sát thấy thùy nhộng (CV) với bể lớn dãn rộng
(dấu sao)
Plane at level of Biparietal Diameter
The sonographic landmarks identifying the correct BPD plane have been previously described in
this chapter (Figure 5.2) and include the midline falx, the cavum septae pellucidi and the
thalami. Abnormalities detected in this plane include ventriculomegaly (Figure 5.22 A and B),
holoprosencephaly (Figure 5.14), agenesis of the corpus callosum (Figure 5.23) and septo-optic
dysplasia (Figure 5.24). Other rare intracranial abnormalities, such as tumors, can also be
detected in this plane. Comprehensive evaluation of the fetal central nervous system requires multiple views of the fetal brain from its sagittal, coronal and axial (transverse) views and through the abdominal and transvaginal (when feasible) approach.
Các mốc trên siêu âm giúp xác định đúng mặt cắt đường kính lưỡng đỉnh chuẩn đã
được mô tả ở chương trước (hình 5.2), bao gồm liềm não, vách trong suốt, đồi thị.
Những bất thường phát hiện được trong mặt cắt này bao gồm dãn não thất (hình 5.22
A và B), não thất duy nhất (holoprosencephaly) (hình 5.14), bất sản thể chai (hình
5.23) và loạn sản vách thị (hình 5.24). Những bất thường hiếm gặp khác trong sọ, như
khối u, có thể phát hiện trong mặt cắt này. Để đánh giá toàn diện hệ thống thần kinh
trung ương đòi hỏi nhiều mặt cắt của não từ mặt cắt đứng dọc giữa, mặt phẳng trán,
mặt cắt ngang và có thể đánh giá qua đầu dò bụng và đầu dò âm đạo (khi có thể)

Figure 5.20: Transcerebellar plane of a fetus with spina bifida showing the
posterior fossa changes (Chiari II). Note the obliteration of the cisterna magna
(CM) and abnormal shape of the cerebellum (arrows).
Hình 5.20: Mặt cắt ngang tiểu não của thai nhi có chẻ đôi đốt sống cho thấy hố
sau có sự thay đổi (Chiari II) Chú ý: có sự tắc nghẽn bể lớn hố sau (CM) và bất
thường hình dạng tiểu não (mũi tên)

Figure 5.21 A and B: Longitudinal (Mid-sagittal) planes of the fetal spine in 2 fetuses (A and B) with spina bifida.
Note the lumbo-sacral locations of the spinal defects (arrows).
Hình 5.21 A và B: Mặt cắt đứng dọc giữa của cột sống ở 2 thai (A và B) có chẻ đôi đốt sống. Chú ý vị trí thắt lưngcùng của khiếm khuyết đốt sống (mũi tên)

Figure 5.22 A and B: Transverse plane of the fetal head) in 2 fetuses with bilateral ventriculomegaly
(asterisks). Note the enlarged lateral ventricles (asterisks).
Hình 5.22 A và B: Mặt cắt ngang đầu ở 2 thai có não thất bên 2 bên dãn rộng (dấu sao).
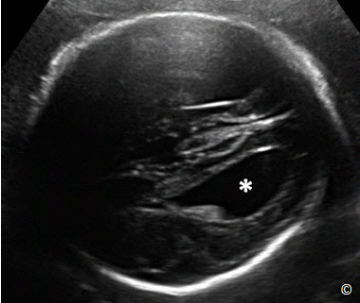
Figure 5.23: Transverse plane of the fetal head at the
level of the lateral ventricles in a fetus with agenesis
of the corpus callosum (ACC). Note the tear-shaped
lateral ventricle (asterisk), a characteristic of ACC.
Hình 5.23: Mặt cắt ngang não thất bên ở thai có bất
sản thể chai (ACC). Chú ý: hình ảnh não thất bên dãn
hình giọt nước (dấu sao), 1 đặc điểm đặc trưng của bất
sản thể chai

Figure 5.24: Transverse plane of the fetal head at the level
of the BPD in a fetus with septo-optic dysplasia. Note the
absence of cavum septae pellucidi and fusion of frontal
horns of the lateral ventricles (arrows). LV= left ventricle.
Hình 5.24: Mặt cắt ngang lưỡng đỉnh có loạn sản vách-thị.
Chú ý: không quan sát thấy vách trong suốt và sừng trán não
thất bên 2 bên thông nhau (mũi tên). LV= não thất bên trái.
Facial Anatomy
Basic sonographic anatomy of the face can be primarily achieved by the evaluation of the orbits
and the upper lip and philtrum.
Cấu trúc giải phẫu ta có thể đánh giá đầu tiên là hai hốc mắt, môi trên và nếp mũi-môi
(nhântrung)
Plane at level of Fetal Face
The evaluation of the fetal face can be obtained by rotating the transducer 90 degrees from the
BPD plane and sliding tangentially to view the two orbits and then the upper lip and philtrum.
The bi-ocular plane is a tangential plane of the fetal head at the level of the orbits (Figure 5.25).
The tangential view of the lips (Figure 5.26) allows for the detection of facial clefting (Figure
5.27). The mid-sagittal view of the facial profile (Figure 5.28) is important as it allows for
evaluation of the fetal lower chin, is recognized by mothers and may play a role in maternal-fetal
bonding.
Để khảo sát vùng mặt thai nhi, từ mặt cắt lưỡng đỉnh, ta xoay đầu dò 90 độ và trượt
nhẹ về phía trước tiếp tuyến với vùng mặt để quan sát 2 hốc mắt, môi trên và nhân
trung. Mặt phẳng ngang hốc mắt là mặt phẳng tiếp tuyến với đầu ở vị trí hốc mắt (hình
5.25). Mặt phẳng tiếp tuyến với môi (hình 5.26) có thể phát hiện chẻ mặt (hình 5.27).
Mặt phẳng đứng dọc giữa mặt (hình 5.28) khá quan trọng do nó cho ta khảo sát được
vùng cằm dưới, giúp các bà mẹ có thể nhận ra con mình và đóng vai trò quan trọng
trong việc làm cầu nối giữa tình cảm mẹ và con

Figure 5.25: Tangential plane of the fetal head at the
level of the orbits. Outer (1) and inner (2) ocular
diameters can be measured in this plane.
Hình 5.25: Mặt phẳng tiếp tuyến của vùng đầu ở ngang
hốc mắt. (có thể đo đường kính ngoài (1) và trong (2)
của hốc mắt ở mặt cắt này)
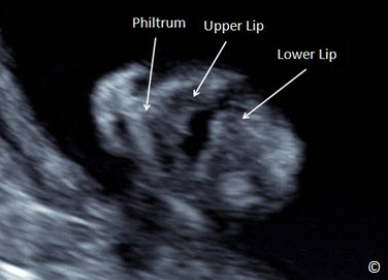
Figure 5.26: Tangential plane of the fetal face showing the
soft tissue of the upper lip, philtrum and lower lip (labeled).
Hình 5.26: Mặt phẳng tiếp tuyến của vùng mặt cho thấy
phần mô mềm của môi trên, nếp mũi môi, và môi dưới (xem
chú thích trên hình

Figure 5.27: Tangential plane of the fetal face showing the soft tissues of the
upper lip, philtrum and lower lip in a fetus with left cleft lip (asterisk).
Hình 5.27: Mặt phẳng tiếp tuyến của vùng mặt cho thấy phần mô mềm của môi
trên, nếp mũi-môi, và môi dưới ở thai nhi có sứt môi (dấu sao)

Figure 5.28: Midsagittal view of the fetal head and face. Note the
recognizable fetal profile that includes the tip of the nose, the upper lip,
and lower lip (labeled).
Hình 5.28: Mặt cắt đứng dọc giữa của vùng đầu và mặt. Chú ý trên hình
mặt cắt nghiêng có thể nhận biết được chóp mũi, môi trên, môi dưới (chú
thích trên hình)
Chest Anatomy
The plane required to assess both the lungs and the heart is the 4-chamber view, which
corresponds to an axial view of the chest at the level of the heart (Figure 5.29). Table 5.9 lists
the sonographic landmarks of the four-chamber view plane.
Mặt cắt cần cho việc khảo sát phổi và tim là mặt cắt 4 buồng, mặt cắt này tương ứng
với mặt cắt ngang của ngực ở vị trí tim. (hình 5.29) Bảng 5.9 nêu ra những điểm mốc
giải phẫu của mặt cắt 4 buồng.
TABLE 5.9 Sonographic Landmarks of the Four-Chamber View Plane
- One full rib on each side of the chest
- Four-chamber view
- Heart occupies 1/3 of thoracic area
- Heart rotated to left with cardiac axis at 45 +/-20o
BẢNG 5.9 Các mốc giải phẫu trên siêu âm của mặt cắt 4 buồng tim
- Toàn bộ phần cung sườn ở mỗi bên
- 4 buồng tim
- Tim chiếm 1/3 lồng ngực
- Mỏm tim lệch trái với trục tim nằm trong khoảng 45+/- 20 độ.

Figure 5.29: Axial (transverse) view of the fetal chest at the level of
the four-chamber view. Note the presence of one full rib on each
lateral border (Rib). S= spine, LA= left atrium, RA= right atrium, LV=
left ventricle and RV= right ventricle.
Hình 5.29: Mặt cắt ngang ngực ở ngang vị trí 4 buồng tim. Chú ý: ta có
thể thấy trọn cung xương sườn ở mỗi bên trên hình này (Rib). S= spine:
cột sống, LA= left atrium: nhĩ trái, RA= right atrium: nhĩ phải, LV= left
ventricle: thất trái and RV= right ventricle: thất phải.
In this plane, the cardiac chamber that is the most posterior is the left atrium, whereas the cardiac
chamber just below the sternum is the right ventricle (Figure 5.29). Major anomalies that can be
identified in this view include cardiac and pulmonary malformations. Common congenital heart
abnormalities that can be detected on the 4-chamber view include ventricular hypoplasia (right or
left) (Figure 5.30), large septal defects (atrio-ventricular septal defect) and severe outflow tract
obstructions (pulmonary valvular atresia or critical aortic stenosis).
Trong mặt cắt này, buồng tim nằm sau nhất là tâm nhĩ trái, ngược lại, buồng tim nằm
ngay dưới xương ức là tâm thất phải (Hình 5.29). Những bất thường lớn có thể xác
định ở mặt cắt này bao gồm những bất thường tim và phổi. Những bất thường bẩm sinh tim thường gặp có thể phát hiện trên mặt cắt 4 buồng bao gồm thiểu sản tim (trái hoặc phải) (Hình 5.30), bất thường lá van lớn (kênh nhĩ thất) và tắc nghẽn buồng thoát nặng (không lỗ van động mạch phổi hoặc hẹp đáng kể động mạch phổi).
Most of these cardiac defects
require neonatal cardiac surgery because of ductus-dependency. Atrio-ventricular septal defect
does not represent a neonatal emergency, but is associated with Down syndrome in up to 60% of
the cases. Most common chest lesions include: diaphragmatic hernia (Figure 5.31); cystic and
hyperechoic lesions of the lung, such as Congenital Cystic Adenomatoid Malformation (C-CAM,
cystic or solid type) (Figure 5.32); extra-lobar sequestration (Figure 5.33); and pleural effusions
(Figure 5.34).
Hầu hết
những bất thường tim này cần can thiệp phẫu thuật sớm sau sanh do phụ thuộc ống
động mạch. Kênh nhĩ thất không phải là bênh lí cần can thiệp khẩn sau sanh nhưng nó
kết hợp với hội chứng Down trong 60% các trường hợp. Hầu hết các tổn thương lồng
ngực thường gặp bao gồm: thoát vị hoành (Hình 5.31); tổn thương tăng sinh dạng
nang và tăng sáng phổi như trong bệnh lí tăng sinh tuyến dạng nang (CCAM, thể nang
hoặc đặc) (hình 5.32); phổi biệt trí thể ngoại thùy (extra-lobar sequestration) (Hình
5.33); và tràn dịch màng phổi (hình 5.34).
Some of these lesions are benign and often regress spontaneously by the time of
birth. Pleural effusions, if in the context of non-immune hydrops fetalis, can lead to fetal or
neonatal demise. Diaphragmatic hernia needs early post-natal surgery, with survival rates of
roughly 50 - 70% in tertiary centers.
Một vài tổn thương này là lành tính và
thường thoái hóa tự nhiên lúc gần sanh. Nếu tràn dịch màng phổi xảy ra trong bệnh
cảnh thai tích dịch không do nguyên nhân miễn dịch, thì nó có thể dẫn đến tử vong
trong bào thai hoặc sau sanh. Thoát vị hoành cần mổ sớm sau sanh, với tỉ lệ sống sót
khoảng 50-70% nếu được mổ ở tuyến trên có đủ trang thiết bị và chuyên môn.
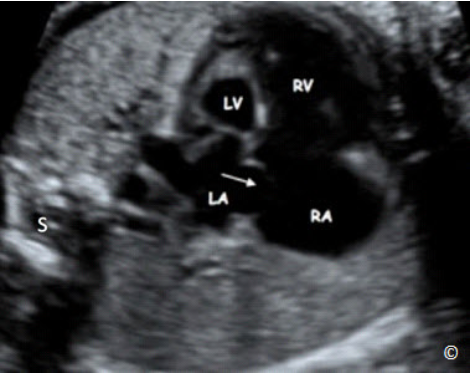
Figure 5.30: Four-chamber view plane of a fetus with hypoplastic left heart syndrome. Note the
diminutive size of the left ventricle (LV). Arrow points to the foramen ovale that typically displays
reverse flow in this condition. S = spine, LA= left atrium, RA= right atrium, and RV= right ventricle.
Hình 5.30: mặt cắt 4 buồng của thai nhi có hội chứng thiểu sản tim trái. Chú ý kích thước thất trái
nhỏ (LV). Trong trường hợp này, mũi tên chỉ lỗ bầu dục, nơi có dòng phụt ngược điển hình trong
trường hợp này. S = spine: cột sống, LA= left atrium: nhĩ trái, RA= right atrium: nhĩ phải, and RV=
right ventricle: thất phải.

Figure 5.31: Transverse plane of the chest in a fetus with congenital
diaphragmatic hernia. Note the upward displacement of the stomach
(St) into the chest. The heart (labeled) is pushed into the right chest. S
= spine, R=right, L=left.
Hình 5.31: Mặt cắt ngang ngực ỏ thai nhi có thoát vị hoành. Chú ý: dạ
dày (St) đi lên trên lồng ngực. Tim bị đẩy sang phải lồng ngực. S = spine:
cột sống, R=phải, L=trái.

Figure 5.32: Transverse plane of the fetal chest at the level of the four-chamber view in a fetus
with congenital cystic adenomatoid malformation of the left lung. Note the large echogenic lung
mass (arrows) associated with fetal ascites (asterisk). The heart is shifted to the right chest. R =
right, L = left and S = spine.
Hình 5.32: Mặt cắt ngang ngực qua 4 buồng tim ở thai nhi có tăng sinh tuyến dạng nang bẩm sinh
của phổi trái. Chú ý khối echo dày sáng lớn kết hợp với tràn dịch (dấu sao). Tim bị đẩy lệch sang
ngực phải. R = phải, L = trái and S = cột sống.

Figure 5.33: Transverse plane of the chest in 2D and color Doppler
modes in a fetus with pulmonary sequestration (white arrows). Note
the vascular supply (yellow arrow) that typically arises from the
systemic circulation. S = spine
Hình 5.33: Mặt cắt ngang ngực ở siêu âm 2D và siêu âm Doppler màu
ở thai nhi có phổi biệt trí (mũi tên trắng). Chú ý mạch máu cung cấp
(mũi tên vàng) thường xuất phát từ tuần hoàn hệ thống. S= cột sống.

Figure 5.34: Transverse view of the fetal chest at 23 weeks’
gestation showing bilateral pleural effusions (arrows). Pleural
effusions regressed spontaneously and resolved in this fetus with
follow-up ultrasound examinations. S = spine, RL = right lung, LL =
left lung.
Hình 5.34: Mặt cắt ngang ngực ở tuổi thai 23 tuần cho thấy tràn dich
màng phổi 2 bên (mũi tên). Tràn dịch màng phổi thoái hóa tự nhiên
và hấp thu trong những lần siêu âm theo dõi sau đó. S = cột sống, RL
= phổi phải, LL = phổi trái.
Abdominal Anatomy
The stomach is visualized on the transverse view in which the AC is measured. Persistent, nonvisualization of the stomach is typically a sign of esophageal atresia, whereas double bubble is a
sign of duodenal atresia (Figure 5.35). Wall abnormalities include exomphalos (omphalocele)
(Figure 5.36) and gastroschisis (Figure 5.37 A and B).
Dạ dày thấy được ở mặt cắt chuẩn ngang bụng, đó cũng là mặt cắt dùng để đo chu vi
bụng (CVB). Nếu vẫn không quan sát thấy dạ dày sau nhiều lần khảo sát, thì đó là dấu
hiệu điển hình của teo hẹp thực quản (một đoạn của thực quản không có lỗ thông),
ngược lại nếu thấy hình ảnh bóng đôi, là dấu hiệu của teo hẹp tá tràng. (Hình 5.35).
Những bất thường thành bụng bao gồm thoát vị rốn (hình 5.36) và hở thành bụng
(hình 5.37 A và B).
All these anomalies are usually non-life
threatening, but require early neonatal surgery. Some major kidney anomalies are associated with
significant decrease in amniotic fluid such as bilateral renal agenesis (Figure 5.38 A and B),
infantile polycystic disease (Figure 5.39 A - C), and bladder outlet obstruction (Figure 5.40 A
and B). Hydronephrosis, from reflux or pyelo-ureteral obstruction (Figure 5.41) is generally less
severe.
Tất cả những bất thường thường không đe dọa tính mạng, nhưng
đòi hỏi phải phẫu thuật sớm sau sanh. Một vài bất thường lớn thường kết hợp lượng
nước ối giảm nhiều như bệnh lí bất sản thận 2 bên (Hình 5.38 A và B), bệnh lí thận đa
nang ở trẻ nhỏ (Figure 5.39 A - C), và tắc nghẽn đường ra của bàng quang (Hình 5.40
A và B). Thận ứ nước, do trào ngược hoặc tắc nghẽn bể thận-niệu quản (hình 5.41)
nhìn chung thường ít nghiêm trọng hơn.

Figure 5.35: Transverse plane of the abdomen in a
fetus with duodenal atresia. Note the enlarged
stomach that crosses the midline (dashed line) and
is shaped in a double bubble (asterisks). S = spine.
Hình 5.35: mặt cắt ngang bụng với hình ảnh teo hẹp
thực quản. Chú ý dạ dày to vượt qua đường giữa
(đường gạch nối) và có hình ảnh bóng đôi (dấu sao).
S= cột sống.

Figure 5.36: Transverse plane of the fetal abdomen in a fetus
with an omphalocele (O). Note the central location of the
defect in the abdomen (arrows). S = spine.
Hình 5.36: cho thấy ở mặt cắt ngang bụng có hình ảnh thoát vị
rốn (O). Chú ý vị trí trung tâm của khiếm khuyết thành bụng
(mũi tên). S = cột sống.

Figure 5.37 A and B: Transverse (A) and midsagittal (B) planes of a fetus with gastroschisis (G). Note the
lack of a membrane cover of the gastroschisis (arrows). AC = Abdominal Circumference.
Hình 5.37 A và B: Mặt phẳng cắt ngang (A) và mặt phẳng đứng dọc giữa (B) của thai nhi có hở thành bụng (G). Chú ý khối
thoát vị không có màng bao (mũi tên). AC = Abdominal Circumference (chu vi vòng bụng)

Figure 5.38 A and B: Coronal planes of the abdomen in 2D (A) and color Doppler (B) modes in a fetus with
bilateral renal agenesis. Note the presence of anhydramnios (arrows) and absence of kidneys (asterisks) in
the renal fossa. Note the absence of renal arteries on color Doppler (B).
Hình 5.38 A và B: Mặt phẳng đứng dọc ngang của vùng bụng trên siêu âm 2D (A) và có phổ Doppler (B) ở thai
có bất sản thận 2 bên. Chú ý: không quan sát thấy nước ối (mũi tên) và không thấy thận ở 2 hố thận (dấu sao)
ở cả 2 hình ảnh trên. Không thấy động mạch thận 2 bên trên siêu âm Doppler (B)

Figure 5.39 A, B, and C: Transverse (A) and longitudinal (B and C) views of the kidneys in a fetus
with infantile polycystic kidney disease. Note the enlarged size of both kidneys and increase in
echogenicity. There is also associated anhydramnios (not shown).
Hình 5.39 A, B, và C: Mặt cắt ngang (A) và dọc (B và C) của 2 thận ở thai nhi có bệnh lí thận đa
nang ở trẻ em. Chú ý sự gia tăng kích thước thận 2 bên và 2 thận tăng phản âm. Đồng thời có kèm
vô ối trong trường hợp này (không thấy trong hình).

Figure 5.40 A and B: Transverse planes of the lower (A) and upper (B) pelvis in a fetus with posterior
urethral valves. Note the distended bladder (B), dilated ureters, seen on cross section in A (U) and the
characteristic keyhole appearance of the proximal urethra, seen in A (asterisk).
Hình 5.40 A và B: mặt cắt ngang phía dưới (A) và trên (B) vùng chậu với van niệu đạo sau. Chú ý bàng
quang căng to (B), niệu quản dãn, quan sát thấy ở mặt cắt ngang ở hình A (U) và dấu hiệu chìa khóa của
đoạn niệu đạo gần ở hình A (dấu sao)

Figure 5.41: Coronal view of the abdomen in a fetus with bilateral
uretero-pelvic obstruction. Note the dilated renal pelves (asterisks).
The kidney borders are marked with arrows.
Hình 5.41: Mặt cắt đứng dọc vùng bụng cho thấy hình ảnh tắc nghẽn bể
thận niệu quản 2 bên. Chú ý bể thận 2 bên dãn (dấu sao). Giới hạn 2
thận được đánh dấu bằng mũi tên 2 đầu trên hình.
Skeletal Anatomy
The spine should be visualized and evaluated in sagittal, transverse or coronal planes, though the
highest detection rate of spina bifida (Figure 5.42 A - C) is not reached through the direct
assessment of the spine but through the recognition of the cranial signs [“banana” (Figure 5.43)
and “lemon” (Figure 5.44) signs]. The long bones of the 4 limbs should be visualized as well,
noting major abnormalities, such as severe shortening (micromelia) or bowing (Figures 5.45 and
5.46).
Cần khảo sát và đánh giá cột sống ở mặt cắt đứng dọc giữa, mặt cắt ngang hoặc mặt
phẳng trán, mặc dù tỉ lệ phát hiện chẻ đôi đốt sống cao nhất (hình 5.42 A - C chủ yếu
dựa vào các dấu hiệu gián tiếp của não [dấu hiệu “trái chuối” (hình 5.43) và “trái chanh”
(hình 5.44)]. Ta cũng cần khảo sát những xương dài của tay chân, chú ý đến những
bất thường lớn như ngắn chi nặng hoặc cong nhiều ( Hình 5.45 và 5.46).
An attempt to visualize both hands and feet should be made when feasible. Major
abnormalities, such as transverse reduction defect, with absence of a hand or a foot, or aplasia
radii can be diagnosed when such attempt is made. Of importance is also the assessment of fetal
joint movement. Fixed joints in a fetus should suspect the presence of arthrogryposis.
Cần cố gắng
khảo sát tay chân khi có thể. Nhờ đó, có thể chẩn đoán những bất thường lớn, với
khiếm khuyết mất chi như không có bàn tay hoặc bàn chân hoặc bất sản xương quay.
Một điều quan trọng nữa là cần đánh giá sự cử động của các khớp. Nếu có dấu hiệu
cứng các khớp, ta có thể nghĩ đến bệnh lí co cứng khớp.

Figure 5.42 A, B, and C: Mid-sagittal planes of the fetal pelvis (P)(Figure A), abdomen (Ab)(Figure B), chest
(Ch) and neck (N)(Figure C) showing longitudinal views of the spine. The intact overlying skin can be seen
in planes A and B (arrows).
Hình 5.42 A, B, và C: Mặt cắt đứng dọc giữ của khung chậu (P) (hình A), bụng (Ab) (hình B), ngực (Ch) và cổ
(N) (hình C) cho thấy mặt cắt dọc giữa của cột sống. Sự liên tục của nếp da trên mặt cắt A và B (mũi tên).

Figure 5.43: Transverse view of the fetal head at the level of the
cerebellum (Transcerebellar) in a fetus with spinal neural tube defect.
Note the ”banana-shaped” cerebellum (arrows, yellow line), a central
nervous system feature (Arnold Chiari) associated with open neural
tube defect. See text for details.
Hình 5.43: minh họa mặt cắt ngang của tiểu não ở thai nhi có khiếm khuyết ống thần kinh. Chú ý
dấu hiệu tiểu não hình trái chuối ( mũi tên, đường viền màu vàng) là 1 đặc điểm bất thường của hệ
thống thần kinh trung ương (Arnold Chiari) kết hợp với dị tật ống thần kinh hở. Xem chi tiết ở phần
bài viết.

Figure 5.44: Transverse view of the fetal head at the level of the lateral
ventricular plane in a fetus with spinal neural tube defect. Note the
”lemon-shaped” cranium (arrows), a feature (Arnold Chiari) associated
with open neural tube defect. See text for details.
Hình 5.44: Mặt cắt ngang đầu ở vị trí não thất bên có dị tật ống thần kinh.
Chú ý hộp sọ có hình “trái chanh” (mũi tên), là 1 đặc điểm của bất thường
hệ thần kinh trung ương (Arnold Chiari) đi kèm dị tật hở ống thần kinh. Xem
mô tả chi tiết ở phần bài viết.

Figure 5.45: Longitudinal view of the femur in 2D mode (A), and the upper extremity in 3D
ultrasound (B) of a fetus with lethal skeletal dysplasia. Note the severe shortening and bowing
of the long bones.
Hình 5.45: mặt cắt dọc xương đùi trên siêu âm 2D (A), và chi trên ở siêu âm 3D (B) của cùng 1
thai nhi có loạn sản xương gây chết. Chú ý xương dài ngắn rõ và cong nhiều.

Figure 5.46: Midsagittal view of a fetus with lethal skeletal dysplasia (same
as in figure 5-45). Note the small chest (C) in comparison to the abdomen
(A).
Hình 5.46: Mặt cắt đứng dọc giữa của thai nhi có loạn sản xương gây chết
(tương tự như hình 5-45). Chú ý ngực nhỏ (C) so với bụng (A).
REFERENCES:
1) Hadlock FP, Harrist RB, Carpenter RJ, Deter RL, Park SK. Sonographic estimation of
fetal weight. The value of femur length in addition to head and abdomen measurements.
Radiology. 1984 Feb;150(2):535-40
2) Sandmire HF. Whither ultrasonic prediction of fetal macrosomia? Obstetric Gynecology
1993;82:860-862
3) L. J. Salomon, Z. Alfirevic, V. Berghella, C. Bilardo, E. Hernandez-andrade, S. L.
Johnsen, K. Kalache, K.yY Leung, G. Malinger, H. Munoz, F. Prefumo, A. Toi and W.
Lee on behalf of the ISUOG Clinical Standards Committee. Practice guidelines for
performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obstetric
Gynecology 2011; 37: 116–126.
4) ISUOG. Cardiac screening examination of the fetus: guidelines for performing the ‘basic’
and ‘extended basic’ cardiac scan. Ultrasound Obstetric Gynecology 2006; 27: 107–113.
5) ISUOG. Sonographic examination of the fetal central nervous system: guidelines for
performing the ‘basic examination’ and the ‘fetal neurosonogram’. Ultrasound Obstetric
Gynecology 2007; 29: 109–116
6) American Institute of Ultrasound in Medicine practice guidelines on the performance of
the obstetric ultrasound examination, 2013.
http://www.aium.org/resources/guidelines/obstetric.pdf
Nhận xét
Đăng nhận xét