Ultrasound of the Non-Pregnant Uterus
INTRODUCTION
Ultrasound is the most optimal imaging modality for the evaluation of the uterus and should be used first when the patient’s symptoms suggest the presence of uterine or other surrounding organ abnormalities. The approach to imaging the uterus by ultrasound can be accomplished by the transabdominal or the transvaginal route and is typically dictated by the type of uterine pathology being evaluated. With the exception of large uterine masses, such as uterine
leiomyomas, which extend the uterus outside of the pelvis, the transvaginal approach, with its
higher resolution and closer proximity to pelvic organs, is preferred, as it enhances the
sonographic depiction of normal and abnormal uterine anatomy. Furthermore, the transvaginal
transducer allows for direct contact with pelvic tissue and thus can elicit pain or discomfort
during the ultrasound examination and thus correlate the patient’s symptoms with the
sonographic findings.
Siêu âm là phương tiện hình ảnh tối ưu nhất để đánh giá tử cung. Siêu âm nên được chỉ định
đầu tiên khi bệnh nhân có những triệu chứng gợi ý bất thường ở tử cung hoặc các cơ quan lân
cận. Siêu âm tử cung có thể thực hiện qua ngã bụng hoặc ngã âm đạo, việc lựa chọn chỉ định
dựa vào bệnh lý của tử cung. Ngoại trừ các khối u tử cung to vượt ra khỏi vùng chậu thì siêu
âm ngã âm đạo được ưa chuộng hơn vì có độ phân giải cao và gần với các cơ quan vùng chậu
hơn, giúp hiển thị hình ảnh giải phẫu siêu âm của tử cung tốt hơn. Hơn nữa, siêu âm với đầu dò
âm đạo cho phép tiếp xúc trực tiếp với các mô vùng chậu, vì vậy có thể phát hiện cảm giác đau
hoặc khó chịu của bệnh nhân trong quá trình thăm khám, từ đó liên hệ các triệu chứng lâm
sàng của bệnh nhân với các dấu hiệu trên siêu âm.
When the transvaginal approach is not feasible, the transrectal or the
translabial approach can be used. This chapter discusses and illustrates the sonographic features
of the normal non-pregnant uterus and the most common uterine and endometrial malformations.
Khi không thể thực hiện siêu âm ngã âm
đạo được thì có thể dùng ngã trực tràng (transrectal) hoặc ngã môi bé (translabial). Trong
chương này sẽ thảo luận và minh họa về các phương thức siêu âm tử cung không mang thai
bình thường, các dị dạng tử cung và nội mạc tử cung thường gặp nhất.
PREPARATION FOR THE EXAMINATION
CHUẨN BỊ BỆNH NHÂN
Given that the majority of the ultrasound examinations to assess the uterus can be performed
with the transvaginal approach, it is recommended that the patient present with an empty bladder.
The patient is best placed in a dorsal lithotomy position, with the legs flexed and the perineum at
the edge of table, which allows for manipulation of the transvaginal transducer. The transvaginal
transducer is best introduced under real-time imaging, and the presence of a chaperone should be
considered in accordance with local policies.
Siêu âm đánh giá tử cung phần lớn được thực hiện qua ngã âm đạo vì vậy bệnh nhân nên đi
tiểu sạch trước khi siêu âm để bàng quang trống. Bệnh nhân nằm tư thế sản khoa với hai chân co
lại và tầng sinh môn nằm sát mép dưới bàn siêu âm để người thực hiện có thể thao tác dễ dàng
với đầu dò âm đạo. Hình ảnh được hiển thị ở chế độ thời gian thực. Cần có sự hiện diện của
người thứ 3 trong suốt quá trình siêu âm.
When a transabdominal ultrasound is performed,
the patient’s bladder should be distended adequately to displace small bowel from the field of
view. A written request for the ultrasound examination should be available and should provide
sufficient clinical information to allow for the appropriate performance and interpretation of the
examination (1). Refer to chapter 13 for more details on the technical aspects of the transvaginal
ultrasound examination. Indications for the examination of the pelvis by ultrasound are listed in
Table 11.1.
Khi thực hiện siêu âm ngã bụng, bàng quang bệnh
nhân phải căng để đẩy ruột non ra khỏi vùng cần khảo sát. Cần có phiếu chỉ định siêu âm
cung cấp đầy đủ các thông tin lâm sàng cần thiết để việc thực hiện siêu âm chính xác và phù
hợp (1). Xem chương 13 để biết thêm chi tiết về kỹ thuật siêu âm qua ngã âm đạo. Các chỉ
định siêu âm vùng chậu được liệt kê trong Bảng 11.1.
Table 11.1
Indication of Pelvic Sonography Include, but are not Limited to the Following:
[Modified with permission from the American Institute of Ultrasound in
Medicine (1)]
- Pelvic pain
- Dysmenorrhea (painful menses)
- Amenorrhea (absence of menses)
- Menorrhagia (excessive menstrual bleeding)
- Metrorrhagia (irregular uterine bleeding)
- Menometrorrhagia (excessive irregular uterine bleeding)
- Follow-up of a previously detected abnormality
- Evaluation, monitoring, and/or treatment of infertility patients
- Delayed menses, precocious puberty, or vaginal bleeding in a prepubertal child
- Postmenopausal bleeding
- Abnormal or technically limited manual pelvic examination
- Signs or symptoms of pelvic infection
- Further characterization of a pelvic abnormality noted on another imaging study
- Evaluation of congenital uterine anomalies
- Excessive bleeding, pain, or signs of infection after pelvic surgery, delivery, or abortion
- Localization of an intrauterine contraceptive device
- Screening for malignancy in patients at increased risk
- Urinary incontinence or pelvic organ prolapse
- Guidance for interventional or surgical procedures
BẢNG 11.1 Các chỉ định siêu âm vùng chậu [Có sửa đổi dưới sự cho phép của Viện siêu
âm y khoa Mỹ (1)]
- Đau vùng chậu
- Thống kinh
- Vô kinh
- Rong kinh
- Rong huyết
- Xuất huyết tử cung bất thường
- Theo dõi bất thường đã phát hiện trước đó
- Đánh giá, theo dõi, và/hoặc điều trị vô sinh
- Dậy thì muộn, dậy thì sớm, hoặc xuất huyết âm đạo ở trẻ chưa dậy thì
- Xuất huyết hậu mãn kinh
- Thăm khám vùng chậu bằng tay có bất thường hoặc hạn chế
- Có triệu chứng viêm nhiễm vùng chậu
- Đánh giá sâu hơn những bất thường ở vùng chậu được ghi nhận trên các phương pháp
khảo sát hình ảnh khác
- Đánh giá các dị dạng tử cung bẩm sinh
- Chảy máu nặng, đau hoặc triệu chứng nhiễm trùng sau phẫu thuật vùng chậu, sau sanh
hoặc sẩy thai
- Xác định vị trí dụng cụ tử cung
- Tầm soát bệnh ác tính ở những bệnh nhân nguy cơ cao
- Tiểu không kiểm soát hoặc sa tạng chậu
- Dẫn đường cho các can thiệp hoặc thủ thuật
SCANNING TECHNIQUES
KỸ THUẬT KHẢO SÁT
The sonographic examination of the uterus by the transvaginal approach is typically initiated at
the midsagittal plane. This view is obtained by introducing the transvaginal transducer into the
upper vaginal fornix while maintaining the reference notch on the transducer at the 12 o’clock
position (Figure 11.1). In this view, the uterine fundus, uterine isthmus and cervix is seen
(Figure 11.2) and the uterine length is measured from the fundus to the external os (Figure
11.2). The depth (height) of the uterus (anteroposterior dimension) is measured in the same longaxis view from its anterior to posterior walls, perpendicular to the length (Figure 11.2).
Siêu âm tử cung qua ngã âm đạo thường được bắt đầu bằng mặt cắt dọc giữa (midsagittal).
Hình ảnh thu được bằng cách đưa đầu dò vào vòm trên âm đạo với điểm đánh dấu ở vị trí 12
giờ (Hình 11.1). Trong hình Hình 11.2, chúng ta quan sát được đáy, eo và cổ tử cung và đo
chiều dài tử cung từ đáy đến lỗ ngoài cổ tử cung. Tương tự, bề dày (bề cao) của tử cung
(đường kính trước sau) được đo từ thành trước đến thành sau tử cung vuông góc với chiều dài
tử cung (Hình 11.2).
This midsagittal view also allows for assessment and measurement of the endometrium. The
endometrium should be analyzed for thickness, focal abnormalities, and the presence of fluid in
the endometrial cavity. Measurement of the endometrium should include the anterior and
posterior portions while excluding any endometrial fluids (Figure 11.3). Accurate evaluation and
measurement of the endometrium is important especially in the presence of uterine bleeding.
Mặt cắt dọc giữa này cũng cho phép đánh giá và đo nội mạc tử cung.
Cần lưu ý bề dày nội mạc, các bất thường khu trú và sự hiện diện của dịch trong lòng tử cung.
Đo nội mạc bao gồm phần trước và phần sau trừ đi lớp dịch trong lòng tử cung (nếu có)
(Hình 11.3). Đánh giá và đo nội mạc chính xác đặc biệt quan trọng trong trường hợp có xuất
huyết tử cung.
When measuring endometrial thickness on ultrasound, it is critical to ensure that the uterus is in a
mid-sagittal plane, the whole endometrial lining is seen from the fundal region to the endocervix,
the thickest portion is measured and the image is clear and magnified (Figure 11.3). Rotating the
transducer 90 degrees counterclockwise (maintains correct orientation) allows for the display of
the transaxial or transverse view of the uterus. The operator should fan the probe in the superior
– inferior direction until the widest transverse view of the uterus is displayed (Figure 11.4).
From this widest transverse view, the maximum width of the uterus is measured (Figure 11.4).
Khi đo nội mạc dày trên siêu âm, cần phải đo ở mặt phẳng dọc giữa, toàn bộ
đường nội mạc quan sát được từ vùng đáy tử cung đến cổ trong, đo phần dày nhất, hình ảnh
được phóng to và rõ ràng (Hình 11.3). Xoay đầu dò 90 độ ngược chiều kim đồng hồ (nhằm
duy trì định hướng chính xác) cho phép hiển thị trục ngang của tử cung. Người thực hiện siêu
âm nên quét đầu dò theo hướng từ trên xuống dưới cho đến khi thu được hình ảnh tử cung
rộng nhất theo trục ngang (Hình 11.4). Từ mặt cắt ngang rộng nhất có thể đo được bề rộng
lớn nhất của tử cung (Hình 11.4)
Table 11.1
Indication of Pelvic Sonography Include, but are not Limited to the Following:
[Modified with permission from the American Institute of Ultrasound in
Medicine (1)]
- Pelvic pain
- Dysmenorrhea (painful menses)
- Amenorrhea (absence of menses)
- Menorrhagia (excessive menstrual bleeding)
- Metrorrhagia (irregular uterine bleeding)
- Menometrorrhagia (excessive irregular uterine bleeding)
- Follow-up of a previously detected abnormality
- Evaluation, monitoring, and/or treatment of infertility patients
- Delayed menses, precocious puberty, or vaginal bleeding in a prepubertal child
- Postmenopausal bleeding
- Abnormal or technically limited manual pelvic examination
- Signs or symptoms of pelvic infection
- Further characterization of a pelvic abnormality noted on another imaging study
- Evaluation of congenital uterine anomalies
- Excessive bleeding, pain, or signs of infection after pelvic surgery, delivery, or abortion
- Localization of an intrauterine contraceptive device
- Screening for malignancy in patients at increased risk
- Urinary incontinence or pelvic organ prolapse
- Guidance for interventional or surgical procedures

Figure 11.1: Initial step in the performance of the transvaginal ultrasound examination.
Note that the transvaginal transducer is introduced into the vaginal canal with the
transducer marker at the 12 o’clock position. A mannequin is used for demonstration.
Hình 11.1: Bước đầu tiên trong siêu âm qua ngã âm đạo. Lưu ý rằng đầu dò
được đưa vào âm đạo với điểm đánh dấu (transducer marker) ở vị trí 12 giờ. Mô
hình được sử dụng để minh họa.

Figure 11.2: Midsagittal plane of the uterus showing the uterine fundus, isthmus, cervix
and a collapsed bladder anteriorly (all labeled). In this plane uterine length (Ut-L) and
height (Ut-H) are measured.Chapter 11: Ultrasound of the Non-Pregnant Uterus 215
Hình 11.2: Mặt cắt dọc giữa tử cung cho thấy đáy (Fundus), eo (Isthmus), cổ tử
cung (Cervix) và bàng quang (Bladder) xẹp ở phía trước. Ở mặt cắt này đo được
chiều dài tử cung (Ut-L) và chiều cao tử cung Ut-H)

Figure 11.3: Endometrial thickness measurement. Note that the endometrial thickness is
measured at its thickest portion and in a midsagittal plane of the uterus. See text for details.
Hình 11.3: Đo bề dày nội mạc tử cung. Lưu ý rằng bề dày nội mạc được đo ở chỗ dày
nhất và ở mặt cắt dọc giữa (Midsagittal plane) tử cung.

Figure 11.4: Transverse plane of the uterus at its widest dimensions. In this plane uterine width
(Ut-W) is measured.
Hình 11.4: Mặt cắt ngang tử cung ở vị trí có đường kính rộng nhất. Ở mặt cắt này đo
được chiều rộng tử cung (Ut-W)
During each ultrasound examination, the uterus should be evaluated for its dimensions (including
the endometrium), shape and orientation. The presence of abnormalities involving the cervix,
endometrium and myometrium should be evaluated and reported. Adjunct imaging modalities
such as color and pulsed Doppler can occasionally help in the presence of abnormal findings.
Applying gentle pressure on the transducer while using the other hand on the patient’s abdomen
to exert counter pressure may help to elicit symptoms in presence of endometritis, endometriosis
and pelvic inflammatory disease. This maneuver may also allow assessing for uterine mobility,
which is limited in presence of adhesions or scarring.
Trong mỗi lần siêu âm, nên đánh giá kích thước tử cung (bao gồm cả nội mạc), hình dạng và
chiều hướng tử cung. Các bất thường của cổ tử cung, nội mạc và cơ tử cung nên được đánh
giá và ghi nhận lại. Các phương thức hình ảnh hỗ trợ như Doppler xung và Doppler màu có
thể giúp phát hiện thêm những dấu hiệu bất thường. Đẩy nhẹ nhàng đầu dò kết hợp với ấn
trên bụng bệnh nhân theo hướng ngược lại để tìm các triệu chứng gợi ý viêm nội mạc tử
cung, lạc nội mạc tử cung hoặc viêm nhiễm vùng chậu. Động tác này cũng cho phép đánh giá
độ di động của tử cung trong trường hợp dính hoặc sẹo.
Sonohysterography may be useful for the
assessment of the endometrial cavity when an abnormality is suspected (2) (Figure 11.5).
Sonohysterography (hydrosonography) is performed by inserting a thin, sterile, plastic catheter
(insemination catheter or a small feeding tube), connected to a plastic syringe containing sterile
saline, into the uterine cavity through the cervical canal (Figure 11.6).
Siêu âm bơm nước buồng tử cung
(Sonohysterography, Hydrosonography) có thể giúp đánh giá lòng tử cung trong trường hợp
nghi ngờ có bất thường (2) (Hình 11.5). Siêu âm bơm nước buồng tử cung được thực hiện
bằng cách đưa một catheter nhựa vô trùng mỏng (catheter bơm tinh trùng hoặc ống nuôi ăn
nhỏ), có gắn ống tiêm chứa nước muối vô trùng, đưa ống thông vào buồng tử cung qua kênh
cổ tử cung (Hình 11.6).
The author recommends
performing the procedure during the proliferative phase of the menstrual cycle to avoid the risk
of a pregnant uterus and to ensure a thin endometrium. Other recommendations for
sonohysterography to consider include wiping the external cervical os with an aseptic solution
before inserting the catheter to minimize the risk of infection and flushing the catheter with
saline before insertion to avoid injecting air into the endometrial cavity, which may obscure
visualization. The catheter can be inserted easily through the internal cervical os in most women
but when cervical stenosis is encountered, the use of a tenaculum to straighten the cervix and a
small uterine sound may help in widening the endocervical canal.
Các tác giả khuyến cáo thực hiện thủ thuật trong giai đoạn tăng sinh
của chu kỳ để tránh tử cung có thai và nội mạc tử cung mỏng. Một số khuyến cáo khác bao
gồm lau lỗ ngoài cổ tử cung bằng dung dịch sát khuẩn trước khi đưa catheter vào buồng tử
cung nhằm hạn chế nguy cơ nhiễm trùng và rửa catheter bằng nước muối để tránh bơm khí
vào buồng tử cung làm che khuất tầm nhìn. Catheter được đưa dễ dàng qua lỗ trong cổ tử
cung trong hầu hết các trường hợp, tuy nhiên khi gặp cổ tử cung chít hẹp thì dùng kẹp
(tenaculum) kéo thẳng cổ tử cung và nong bằng ống nhỏ giúp mở rộng kênh cổ tử cung.
Side effects of sonohysterography are rare and include around a 1% risk for endometritis and a 1-5 % risk for significant cramping or pain (3). Taking Ibuprofen orally, 1 hour before the procedure, may help to minimize uterine cramping.
Các tác dụng phụ của siêu âm bơm nước lòng tử cung rất hiếm xảy ra bao gồm: nguy cơ viêm nội
mạc tử cung khoảng 1%, co thắt và đau bụng 1-5% (3). Cho bệnh nhân uống Ibuprofen 1 giờ
trước thủ thuật giúp hạn chế co thắt tử cung.

Figure 11.5: Sonohysterography of a normal endometrial cavity showing the fundus and isthmus (labeled).
Hình 11.5: Hình ảnh buồng tử cung bình thường trên siêu âm bơm nước buồng tử
cung cho thấy đáy (Fundus) và eo (Isthmus)

Figure 11.6: Supplies needed for sonohysterography include a syringe filled with sterile
normal saline and a thin sterile plastic catheter (labeled). See text for details.
Hình 11.6: Dụng cụ cần thiết trong siêu âm bơm nước buồng tử cung bao gồm một ống tiêm
(Syringe) chứa nước muối sinh lý (Normal Saline) và một catheter nhựa vô trùng (Catheter)
The technical aspect of obtaining the mid-coronal plane of the uterus on three-dimensional
sonography will be discussed later in this chapter in the section on congenital mullerian
malformations.
Khía cạnh kỹ thuật để thu được mặt phẳng trán (mid-coronal plane) của tử cung trên siêu âm
3 chiều sẽ được thảo luận trong chương này ở phần bất thường bẩm sinh ống Müller.
SONOGRAPHIC FEATURES OF THE NORMAL UTERUS
ĐẶC ĐIỂM SIÊU ÂM CỦA TỬ CUNG BÌNH THƯỜNG
The uterus is primarily a muscular organ located in the true pelvis between the urinary bladder
anteriorly and the rectosigmoid colon posteriorly. The space between the uterus and the
rectosigmoid is the posterior cul-de-sac; the most dependent area in the peritoneal cavity where
peritoneal fluid tends to accumulate. In the reproductive years, the endometrium is under the
influence of sexual hormones and undergoes anatomic changes during the woman’s menstrual
cycle.
Tử cung là một tạng cơ nằm trong tiểu khung giữa bàng quang ở phía trước và đại-trực tràng
ở phía sau. Khoảng giữa tử cung và đại-trực tràng là túi cùng sau (posterior cul-de-sac) hay
còn gọi là túi cùng Douglas, đây là nơi thấp nhất của ổ phúc mạc mà các dịch trong ổ bụng
thường đọng ở đó. Trong độ tuổi sinh sản, nội mạc tử cung trải qua những thay đổi giải phẫu
dưới tác dụng của hormon sinh dục trong suốt chu kỳ kinh nguyệt.
As described in the section on scanning techniques, the uterus is first imaged in its long axis on
the midsagittal plane, which is obtained by visualizing the long axis of the echogenic
endometrium. The midsagittal plane allows for the visualization of the uterine fundus, a
significant section of the myometrium, the endometrium in sagittal section, the cervix in sagittal
section, the cul-de-sac, the rectosigmoid and the bladder (Figure 11.7).
Measuring the length, depth (height) and width of the uterus, as described in the prior section, should be part of the pelvic ultrasound examination.
Như đã trình bày trong phần kỹ thuật siêu âm, chúng ta có thể đánh giá nội mạc trên mặt
phẳng dọc giữa tử cung. Mặt phẳng này cho phép quan sát vùng đáy tử cung, phần lớn cơ tử
cung, nội mạc tử cung, cổ tử cung, túi cùng, trực tràng và bàng quang (Hình 11.7). Việc đo
đạc chiều dài, chiều sâu (cao) và chiều rộng của tử cung là một phần trong siêu âm vùng
chậu.
The length of a normal nulliparous uterus is 6 - 8.5 cm and in
multiparous women it is 8 - 10.5 cm (4). The depth (height) of the normal uterus in nulliparous
women is 2 – 4 cm and in multiparous women it is 4 – 6 cm (4). The widest transverse plane of
the uterus measures 3 – 5 cm in nulliparous and 4 – 6 cm in multiparous women (4).
Chiều dài bình thường của tử cung ở phụ nữ chưa sanh từ 6 – 8,5 cm và 8 – 10,5 cm ở
phụ nữ sanh nhiều lần (4). Chiều sâu (cao) bình thường của tử cung ở phụ nữ chưa sanh từ 2
– 4 cm và 4 – 6 cm ở phụ nữ sanh nhiều lần (4). Cắt ngang tử cung ở chỗ rộng nhất đo được
từ 3 – 5 cm ở phụ nữ chưa sanh và 4 – 6 cm ở phụ nữ sanh nhiều lần (4)
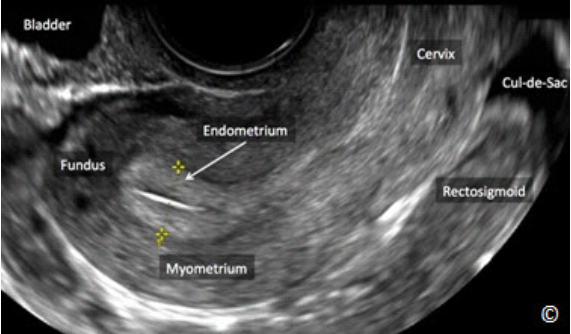
Figure 11.7: Midsagittal plane of the uterus showing the uterine fundus, the myometrium, the endometrium, the cervix, the cul-de-sac, the rectosigmoid and the bladder (all labeled). Note that the myometrium is less echogenic than the endometrium (labeled).
Hình 11.7: Mặt phẳng đứng dọc giữa qua tử cung cho thấy đáy tử cung (Fundus), cơ
tử cung (Myometrium), nội mạc tử cung (Endometrium), cổ tử cung (Cervix), túi cùng
(Cul-de-sac), trực tràng (Rectosigmoid) và bàng quang (Bladder). Lưu ý rằng cơ tử cung
(Myometrium) có hồi âm kém hơn nội mạc tử cung.
It is important to describe and report the orientation of the uterus as part of the ultrasound
examination as this information is helpful if uterine instrumentation is required. The orientation
of the uterus is described in the midsagittal plane and in relation to the supine body. Two terms
are used to describe the orientation of the uterus in the pelvis; flexion and version. Flexion is the
bending of the uterus on itself and thus the uterus is flexed when there is an angle in the
midsagittal plane between the cervix/lower uterine (isthmus) segment and the fundal portion.
Một phần quan trọng trong siêu âm là mô tả hướng tử cung, điều này giúp ích trong trường
hợp cần đo buồng tử cung. Hướng tử cung được mô tả ở mặt phẳng đứng dọc giữa và bệnh
nhân nằm ngửa. Hai thuật ngữ dùng để mô tả hướng tử cung trong khung chậu là gập
(flexion) và ngã (version). Gập là sự uốn cong của tử cung, vì vậy tử cung được gọi là gập
khi có một góc giữa đoạn cổ/đoạn dưới (đoạn eo) tử cung với phần đáy tử cung.
An anteroflexed uterus is a uterus with an acute or obtuse angle (< 180 degrees) between the
cervix/lower uterine (isthmus) segment and the fundus with the fundal portion close to the
bladder (Figure 11.8). A retroflexed uterus is a uterus with a reflex angle (> 180 degrees)
between the cervix/lower uterine (isthmus) segment and the fundus with the fundal portion close
to the rectosigmoid (Figure 11.9).
Tử cung gập trước có đoạn eo và phần đáy tạo với nhau một góc nhọn hoặc tù (<180 độ) và phần đáy tử cung sát với bàng quang (Hình 11.8). Tử cung gập sau có đoạn eo và phần đáy tử cung tạo
với nhau một góc phản (>180 độ)và phần đáy tử cung sát với trực tràng (Hình 11.9)
If there is no angulation between the cervix/lower segment
(isthmus) and the uterine fundus, the uterus is described in terms of version. Version thus
describes displacement of the entire uterus forwards or backwards. An anteverted uterus is a
uterus where the fundal portion is close to the bladder (Figure 11.10) and a retroverted uterus is
a uterus where the fundal region is close to the rectosigmoid (Figure 11.11).
Nếu giữa đoạn eo và phần đáy tử cung không tạo góc thì tử cung được mô tả bằng từ “ngã” nghĩa
là tử cung hướng toàn bộ về phía trước hoặc phía sau. Tử cung ngã trước là tử cung có phần
đáy sát với bàng quang (Hình 11.10) và tử cung ngã sau là tử cung có phần đáy sát với trực
tràng (Hình 11.11)

Figure 11.8: Transvaginal ultrasound of an anteroflexed uterus. Note the obtuse angle (<
180o) between the lower uterine segment (isthmus)/ cervix (A) and the fundal portion (B).
The uterine fundus is close to the bladder (compressed - labeled).
Hình 11.8: Hình ảnh siêu âm qua ngã âm đạo của tử cung gập trước. Lưu ý góc tù (Obtuse
Angle) (<180 độ) giữa đoạn dưới tử cung (eo)/cổ (Cervix) (A) và phần đáy tử cung (Fundus)
(B). Đáy tử cung nằm sát bàng quang (Bladder).

Figure 11.9: Transvaginal ultrasound of a retroflexed uterus. Note the reflex angle (> 180o)
between the lower uterine segment (isthmus) / cervix (A) and the fundal portion (B). The
uterine fundus is close to the rectosigmoid (labeled). Note location of bladder (labeled).
Hình 11.9: Hình ảnh siêu âm qua ngã âm đạo của tử cung gập sau. Lưu ý các góc phản
(Reflex Angle) (>180 độ) giữa đoạn dưới tử cung (eo)/cổ (Cervix) (A) và phần đáy tử cung
(Fundus) (B). Đáy tử cung nằm sát trực tràng (Rectosigmoid). Chú ý vị trí bàng quang
(Bladder).

Figure 11.10: Transvaginal ultrasound of an anteverted uterus. Note the absence of
angulation between the lower uterine segment (isthmus)/ cervix (A) and the fundal
portion (B). The fundal portion is close to the bladder (labeled). Rectosigmoid is labeled.
Hình 11.10: Hình ảnh siêu âm qua ngã âm đạo của tử cung ngã trước. Lưu ý sự vắng mặt
của góc hợp bởi đoạn dưới tử cung (eo)/cổ (Cervix) (A) và phần đáy tử cung (Fundus) (B).
Đáy tử cung nằm sát bàng quang (Baldder).
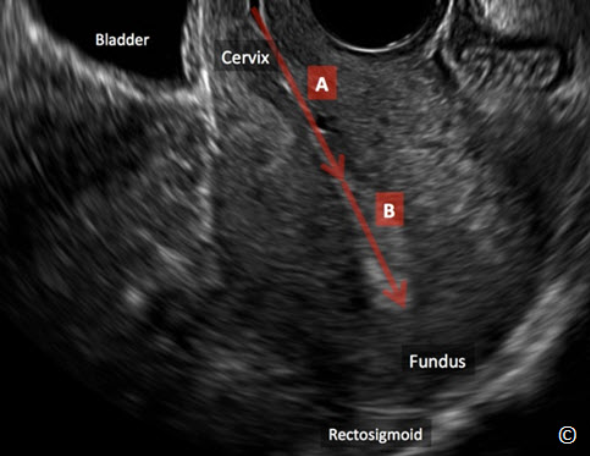
Figure 11.11: Transvaginal ultrasound of a retroverted uterus. Note the absence of
angulation between the lower uterine segment (isthmus)/ cervix (A) and the fundal
portion (B). The fundal portion is close to the rectosigmoid (labeled). Note the location of
the bladder (labeled).
Hình 11.11: Hình ảnh siêu âm qua ngã âm đạo của tử cung ngã sau. Lưu ý sự vắng mặt của
góc hợp bởi đoạn dưới tử cung (eo)/cổ (Cervix) (A) và phần đáy tử cung (B). Đáy tử cung
(Fundus) nằm sát trực tràng (Rectosigmoid). Chú ý vị trí của bàng quang (Bladder).
The myometrium is made of a homogeneous layer of smooth muscle and blood vessels.
Sonographically the normal myometrium is less echogenic than the endometrium (Figure 11.7).
The myometrium can be divided into three layers; the inner or junctional layer, which abuts the
endometrium, is thin and hypoechoic, the middle layer is thick and homogeneous and an outer
layer which is thin and hypoechoic (Figure 11.12). The arcuate vessels separate the middle from
the outer myometrial layers.
Cơ tử cung được cấu tạo bởi một lớp cơ trơn đồng nhất và các mạch máu. Trên siêu âm cơ tử
cung bình thường có hồi âm kém hơn so với nội mạc tử cung (Hình 11.7). Cơ tử cung có thể
được chia thành 3 lớp; lớp trong cùng còn gọi là lớp chuyển tiếp (junctional layer) tiếp giáp
với nội mạc tử cung, hồi âm kém và mỏng, lớp giữa dày và đồng nhất và lớp ngoài cùng hồi
âm kém và mỏng (Hình 11.12). Các mạch máu hình cung nằm giữa lớp ngoài và lớp giữa cơ
tử cung.
The endometrium undergoes significant change during the menstrual cycle (5, 6) and
anatomically is divided into the inner functional layer that sloughs during the menstrual cycle
and the outer basal layer that abuts the myometrial junctional layer. Sonographically, in the
immediate postmenstrual phase, the endometrium appears as a thin echogenic line and typically
measures between 3 – 8 mm (Type A) (Figure 11.13).
Nội mạc tử cung có sự thay đổi đáng kể trong suốt chu kỳ kinh nguyệt (5,6). Về phương diện
giải phẫu, nội mạc tử cung được chia thành 2 lớp: lớp chức năng ở trong sẽ bong ra khi hành
kinh và lớp đáy ở ngoài tiếp giáp với lớp chuyển tiếp của cơ tử cung. Về phương diện siêu
âm, ở giai đoạn ngay sau khi hành kinh, nội mạc tử cung xuất hiện dưới dạng một đường hồi
âm mỏng từ 3 – 8mm (Loại A) (Hình 11.13).
Under the influence of increasing
estradiol hormone levels secreted by the growing ovarian follicles, endometrial proliferation
occurs and endometrial thickening ensues. Sonographically, this is seen as thickening of the
lining into the so-called trilaminar layer (Type B) with an anterior and posterior hypoechoic layer
separated in the midline by an echogenic central line.
Dưới sự ảnh hưởng của nồng độ estrogen ngày
càng tăng được tiết ra từ các nang noãn, nội mạc tử cung tăng sinh và dày lên. Siêu âm nội
mạc tử cung ở giai đoạn này cho hình ảnh 3 lớp với lớp trước và lớp sau hồi âm kém ngăn
cách bởi một đường hồi âm dày ở giữa (Loại B).
During the late proliferative period and
near the time of ovulation, endometrial lining is 8 to 12 mm in thickness with an accentuated
trilaminar appearance (Type C), (Figure 11.14). The post ovulatory endometrial lining, under the
influence of progesterone hormone, secreted by the corpus luteum, is characterized by loss of the
trilaminar appearance and the development of a uniformly hyperechoic endometrium (Type D),
(Figure 11.15).
Ở cuối giai đoạn tăng sinh gần thời điểm
rụng trứng, nội mạc tử cung dày khoảng 8 – 12mm với hình ảnh 3 lớp đặc trưng (Loại C),
(Hình 11.14). Sau khi rụng trứng, dưới sự ảnh hưởng của progesterone tiết ra từ hoàng thể
nội mạc tử cung mất đi hình ảnh 3 lớp đặc trưng và có hồi âm dày đồng nhất (Loại D) (Hình
11.15).

Figure 11.12: Transvaginal ultrasound of a transverse view of the uterus showing the three
myometrial layers. Note the inner thin and hypoechoic layer that abuts the endometrium (labeled),
the middle layer that is thick and homogeneous and the outer layer that is slightly less echogenic than
the middle layer (labeled). Note that the arcuate vessels (labeled) separate the middle from the outer
myometrial layers.
Hình 11.12: Siêu âm đầu dò âm đạo cắt ngang tử cung cho thấy 3 lớp cơ tử cung
(Myometrium). Lưu ý lớp trong (Inner) mỏng và hồi âm kém tiếp giáp với lớp giữa
(Middle) dầy đồng âm và lớp ngoài (Outer) thì hồi âm tương đối kém so với lớp giữa.
Lưu ý các mạch máu hình cung (Arcuate Vessels) nằm giữa lớp ngoài và lớp giữa cơ
tử cung.

Figure 11.13: Transvaginal ultrasound of a sagittal view of the uterus in the immediate
postmenstrual phase. Note the thin echogenic endometrium (labeled). Cervix is labeled for
image orientation. Image is courtesy of Dr. Bernard Benoit.
Hình 11.13: Siêu âm đầu dò âm đạo mặt cắt dọc tử cung ở giai đoạn ngay sau khi hành kinh.
Lưu ý nội mạc tử cung (Endometrium) mỏng. Cổ tử cung (Cervix) được gắn nhãn để định
hướng hình ảnh. Hình ảnh do BS Bernard Benoit cung cấp.
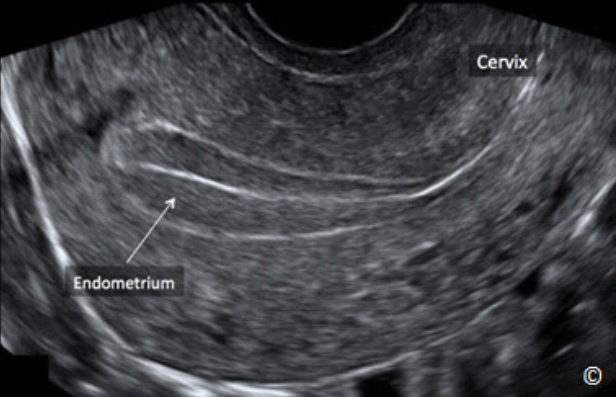
Figure 11.14: Transvaginal ultrasound of a sagittal view of the uterus in the late proliferative,
near ovulation phase of the menstrual cycle. Note the accentuated thick trilaminar
endometrium (labeled). Cervix is labeled for image orientation. Image is courtesy of Dr.
Bernard Benoit.
Hình 11.14: Siêu âm đầu dò âm đạo mặt cắt dọc tử cung ở cuối giai đoạn tăng sinh, gần giai
đoạn rụng trứng của chu kỳ kinh nguyệt. Lưu ý nội mạc tử cung (Endometrium) dày với 3 lớp
rõ rệt. Cổ tử cung (Cervix) được gắn nhãn để định hướng hình ảnh. Hình ảnh do BS Bernard
Benoit cung cấp.
The cervix can be divided into the portio vaginalis or ectocervix, the endocervix and the
endocervical canal. It is best imaged using the transvaginal approach. To fully display the cervix,
the transvaginal transducer is rotated to the midsagittal position, and is pulled gently backward
until the whole cervix comes into view. Applying transducer pressure should be avoided, as it
will distort the cervix. Sonographically, the cervical stroma is of the same consistency as the
myometrium, and is not affected by hormonal changes (7). Nabothian cysts can be occasionally
seen within the cervical stroma (Figure 11.16).
Cổ tử cung có thể chia thành phần trong âm đạo hay cổ ngoài (ectocervix), kênh cổ
(endocervix canal) và cổ trong (endocervix). Cổ tử cung được đánh giá tốt nhất với siêu âm
qua ngã âm đạo. Để hiển thị hình ảnh đầy đủ thực hiện lát cắt đứng dọc giữa và kéo lui nhẹ
nhàng đầu dò cho đến khi thấy được toàn bộ cổ tử cung. Tránh ấn đầu dò vì động tác này sẽ
làm cổ tử cung méo mó. Trên siêu âm, mô cổ tử cung đồng nhất giống như cơ tử cung và
không chịu ảnh hưởng bởi sự thay đổi của nội tiết (7). Thỉnh thoảng có thể thấy những nang
Naboth cổ tử cung (Hình 11.6).

Figure 11.15: Transvaginal ultrasound of a sagittal view of the uterus in the post-ovulatory
phase of the menstrual cycle. Note that the endometrium is uniformly hyperechoic with the
loss of the trilaminar appearance (labeled). Cervix is labeled for image orientation. Image is
courtesy of Dr. Bernard Benoit.
Hình 11.15: Siêu âm đầu dò âm đạo mặt cắt dọc tử cung ở giai đoạn sau rụng trứng của chu
kỳ kinh nguyệt. Lưu ý toàn bộ nội mạc tử cung (Endometrium) hồi âm dày đồng nhất mất cấu
trúc 3 lớp. Cổ tử cung (Cervix) được gắn nhãn để định hướng hình ảnh. Hình ảnh do BS
Bernard Benoit cung cấp

Figure 11.16: Transvaginal ultrasound of the cervix in sagittal view. Note the
presence of a Nabothian cyst (labeled), which typically presents as an anechoic cyst
within the cervical stroma
Hình 11.16: Hình cắt dọc cổ tử cung trên siêu âm ngã âm đạo. Lưu ý nang Naboth
(Nabothian Cyst) thường hiện diện như một nang echo trống ở cổ tử cung.
ADENOMYOSIS
LẠC NỘI MẠC TRONG CƠ TỬ CUNG (ADENOMYOSIS)
Adenomyosis is a common condition that predominantly affects women in the late reproductive
years. It has been noted to occur in about 30% of the general female population and in up to 70%
of hysterectomy specimens depending on the definition of the entity (8). Adenomyosis is defined
by the presence of ectopic endometrial glands and stroma within the myometrium, which induces
a hypertrophic and hyperplastic reaction in the surrounding myometrial tissue.
Lạc nội mạc trong cơ tử cung là một bệnh lý phổ biến gây ảnh hưởng chủ yếu ở những phụ
nữ trong giai đoạn muộn của độ tuổi sinh sản. Tần suất khoảng 30% phụ nữ nói chung và có
khi đến 70% mẫu mô cắt tử cung tùy vào định nghĩa (8). Lạc nội mạc trong cơ tử cung được
định nghĩa là sự hiện diện của tuyến nội mạc tử cung và chất nền trong cơ tử cung gây phản
ứng phì đại và tăng sản mô cơ tử cung xung quanh.
Most patients with adenomyosis are asymptomatic. Symptoms related to adenomyosis include
dysmenorrhea, dyspareunia, chronic pelvic pain and menometrorrhagia. Adenomyosis presents
most commonly as a diffuse disease involving the entire myometrium (Figure 11.17).
Adenomyosis can also present in a focal area of the uterus, known as adenomyoma (Figure
11.18). Adenomyosis is occasionally associated with other uterine pathology such as leiomyoma
and endometrial polyps. Clinical diagnosis of adenomyosis is difficult due to its vague presenting
symptoms. A homogeneously enlarged (globular) uterus on pelvic examination is suggestive of
the diagnosis (Figure 11-17).
Phần lớn bệnh nhân không có triệu chứng. Các triệu chứng của lạc nội mạc trong cơ tử cung
bao gồm thống kinh, đau khi giao hợp, đau vùng chậu mạn tính và rong kinh rong huyết. Lạc
nội mạc trong cơ tử cung hầu hết lan tỏa toàn bộ tử cung (Hình 11.17) nhưng cũng có thể
biểu hiện khu trú ở một vùng của tử cung được gọi là u lạc nội mạc tử cung trong cơ
(adenomyoma) (Hình 11.18). Lạc nội mạc trong cơ tử cung đôi khi kết hợp với các bệnh lý
khác của tử cung như u xơ tử cung và polyp nội mạc tử cung. Chẩn đoán lâm sàng khó khăn
do triệu chứng mơ hồ. Tử cung to đồng nhất (hình cầu) khi khám phụ khoa gợi ý chẩn đoán
(Hình 11.17)

Figure 11.17: Transvaginal ultrasound of the uterus in sagittal view in the presence of
diffuse adenomyosis. Note the globular enlargement of the uterus, the asymmetric
anterior and posterior wall thickness (arrows) and the presence of multiple anechoic
spaces within the myometrium (asterisks). The cervix is labeled for image orientation.
See text and Table 11.2 for more details.
Hình 11.17: Siêu âm tử cung qua ngã âm đạo ở mặt cắt dọc cho thấy hình ảnh lạc nội mạc
trong cơ tử cung lan tỏa. Lưu ý tử cung phì đại hình cầu, thành trước và thành sau dày
không đều (mũi tên) và nhiều khoảng echo trống trong cơ tử cung (dấu hoa thị). Cổ tử
cung (Cervix) được gắn nhãn để định hướng. Xem chi tiết ở Bảng 11.2

Figure 11.18: Transvaginal ultrasound of the uterus in sagittal view in the presence of
focal adenomyosis (arrows). Note the presence of multiple anechoic spaces (arrows)
within the myometrium. See text and Table 11.2 for more details. The cervix is
labeled for image orientation. Image is courtesy of Dr. Bernard Benoit.
Hình 11.18: Siêu âm tử cung qua ngã âm đạo ở mặt cắt dọc cho thấy hình
ảnh lạc nội mạc trong cơ tử cung khu trú (mũi tên). Lưu ý rằng có nhiều
khoảng echo trống trong cơ tử cung. Xem thêm Bảng 11.2. Cổ tử cung
(Cervix) được gắn nhãn để định hướng hình ảnh. Hình ảnh do Dr. Bernard
Benoit cung cấp.
Ultrasound features of adenomyosis have been described in the literature (9) and are listed in
Table 11.2. Figures 11.17 to 11.19 show the common ultrasound features of adenomyosis. The
diagnosis of adenomyosis by ultrasound is best performed by the transvaginal approach and its
clinical implication is most significant in symptomatic women. On some occasions,
differentiating adenomyosis from a leiomyoma may be difficult and color/pulsed Doppler may
be helpful in that setting (10, 11).
Đặc điểm siêu âm của lạc nội mạc trong cơ tử cung đã được mô tả trong y văn (9) và được
liệt kê trong Bảng 11.2. Hình 11.17 đến Hình 11.19 minh họa những đặc điểm siêu âm
thường gặp của lạc nội mạc trong cơ tử cung. Chẩn đoán lạc nội mạc trong cơ tử cung bằng
siêu âm có ý nghĩa đặc biệt quan trọng ở những bệnh nhân có triệu chứng lâm sàng và tốt
nhất nên được thực hiện qua ngã âm đạo. Trong một số trường hợp khó chẩn đoán phân biệt
giữa lạc nội mạc trong cơ tử cung với u xơ tử cung, sử dụng Doppler màu hoặc Doppler xung
có thể giúp ích trong chẩn đoán (10,11).
TABLE 11.2 Ultrasound Findings in Adenomyosis
- Globular enlargement of the uterus
- Anechoic spaces in the myometrium
- Asymmetric anterior and posterior uterine wall thickening
- Subendometrial echogenic linear striations
- Heterogeneous echo texture
- Obscure endometrial-myometrial border
- Thickening of the transition zone
BẢNG 11.2 Đặc Điểm Siêu Âm Của Lạc Nội Mạc Trong Cơ Tử cung
- Tử cung phì đại hình cầu
- Khoảng echo trống trong cơ tử cung
- Thành trước và thành sau tử cung dày không đều
- Những đường hồi âm dày hướng từ nội mạc vào lớp cơ tử cung
- Cấu trúc echo không đồng nhất
- Ranh giới giữa nội mạc và cơ tử cung không rõ ràng
- Vùng chuyển tiếp dày lên

Figure 11.19: Transvaginal ultrasound of the uterus in sagittal view in the presence of
diffuse adenomyosis. Note the globular enlargement of the uterus, the asymmetric
anterior and posterior wall thickness (arrows), the presence of multiple anechoic
spaces within the myometrium (asterisks) and the heterogeneous echo texture. See
text and Table 11.2 for more details.
Hình 11.19: Siêu âm tử cung qua ngã âm đạo cho thấy hình ảnh lạc nội mạc
trong cơ tử cung lan tỏa. Lưu ý tử cung phì đại hình cầu, thành trước và thành
sau dày không đều (mũi tên), có sự hiện diện nhiều khoảng echo trống trong lớp
cơ (dấu hoa thị) và cấu trúc không đồng nhất. Xem chi tiết ở Bảng 11.2
CONGENITAL UTERINE MALFORMATIONS
CÁC DỊ DẠNG BẨM SINH CỦA TỬ CUNG
The true prevalence of female genital tract malformations is unknown (12), but can be up to 8-
10% in women with recurrent pregnancy loss (13). Congenital uterine malformations are
associated with an increased risk of infertility, miscarriage, premature birth, fetal loss, fetal
malpresentation and cesarean sections (14, 15). Accurate diagnosis of the specific type of a
uterine anomaly is of clinical importance as the prognosis and the need for surgical repair is
dependent on this distinction.
Tỷ lệ thực sự của dị tật bẩm sinh đường sinh dục nữ chưa rõ ràng (12), có thể khoảng 8 –
10% ở những phụ nữ sẩy thai liên tiếp (13). Dị dạng bẩm sinh tử cung có liên quan đến tăng
nguy cơ vô sinh, sẩy thai, sanh non, thai lưu, ngôi bất thường và mổ lấy thai (14,15). Chẩn
đoán chính xác loại bất thường tử cung rất quan trọng trong lâm sàng để tiên lượng và cân
nhắc khả năng phẫu thuật.
The American Fertility Society’s classification (1988) consists of
seven basic groups that are based on Mullerian development and its relationship to fertility: (1)
agenesis and hypoplasias, (2) unicornuate uteri, (3) didelphys uteri, (4) bicornuate uteri, (5)
septate uteri, (6) arcuate uteri and (7) anomalies related to diethylstilbestrol exposure syndrome
(16). In this classification, additional findings referring to the vagina, cervix, fallopian tubes,
ovaries and urinary system must be addressed separately.
Theo phân loại của Hiệp hội sinh sản Hoa Kỳ (1988) có 7 nhóm
chính dựa vào sự phát triển của ống Muller và mối quan hệ với khả năng sinh sản: (1) Bất sản
và thiểu sản tử cung (agenesis and hypoplasia), (2) tử cung một sừng (unicornuate uteri), (3)
tử cung đôi (didelphyls uteri), (4) tử cung 2 sừng (bicornuate uteri), (5) tử cung có vách ngăn
(septate uteri), (6) tử cung hình cung (arcuate uteri), (7) các dị dạng liên quan đến hội chứng
phơi nhiễm diethylstilbestrol (16). Trong phân loại này, những bất thường âm đạo, cổ tử
cung, vòi trứng, buồng trứng và hệ niệu được mô tả riêng.
Although transvaginal 2D sonography has been shown to be a good screening tool for the
detection of uterine anomalies with a sensitivity as high as 90 % (17, 18), its ability is limited
however to distinguish between different anomaly types with certainty (19). The development of
three-dimensional (3D) ultrasound has permitted scanning of the uterus in coronal planes, which
allows for accurate depiction of the endometrial and serosal fundus in such planes and thus
allowed for accurate distinction between various types of uterine malformations (Figure 11.20).
Mặt dù siêu âm 2D qua ngã âm đạo được chứng minh là một công cụ sàng lọc tốt các dị dạng
tử cung với độ nhạy đến 90% (17,18), tuy nhiên vẫn còn những hạn chế trong việc chẩn đoán
chính xác loại bất thường tử cung (19). Sự phát triển của siêu âm 3D giúp khảo sát tử cung ở
mặt phẳng trán, điều này cho phép đánh giá chính xác nội mạc và thanh mạc vùng đáy tử
cung ở nhiều mặt phẳng khác nhau nhằm phân biệt chính xác các loại dị tật tử cung (Hình
11.20).
When the uterus is viewed in the midcoronal plane on 3D ultrasound, indentation in the serosal
and endometrial fundus can be seen and measurement of the distance between the mid-fundus
and a line connecting the two internal tubal ostia can be obtained (Figure 11.21). Table 11.3
lists the criteria used by the authors for the classification of congenital uterine malformations by
3D ultrasound.
Trên siêu âm 3D ở mặt phẳng giữa trán (midcoronal plane), chúng ta có thể nhìn rõ
chỗ lồi lõm của thanh mạc và nội mạc vùng đáy tử cung và đo được khoảng cách từ giữa đáy
tử cung đến đường nối giữa 2 lỗ trong của 2 ống dẫn trứng (Hình 11.21). Bảng 11.3 liệt kê
tiêu chí được các tác giả dùng để phân loại dị tật bẩm sinh tử cung trên siêu âm 3D.

Hình 11.20: Hình ảnh tử cung bình thường và bất thường ở mặt phẳng giữa trán trên siêu âm 3D. Lưu ý
hình ảnh rõ ràng của thanh mạc và nội mạc vùng đáy cũng như đoạn dưới tử cung giúp phân biệt các dị
tật ống Muller khác nhau. Xem thêm Bảng 11.3. Chỉnh sửa được sự cho phép của Viện Siêu âm Y khoa
Mỹ (18).
Figure 11.20: Midcoronal planes of uteri obtained from 3-D ultrasound volumes in normal and
abnormal uterine abnormalities. Note the clear depiction of the serosal and endometrial fundi and
lower-uterine segments, which allow for differentiation of various mullerian anomalies. See Table 11.3
for details. Modified with permission from the American Institute of Ultrasound in Medicine (18).

Figure 11.21: Midcoronal plane of the uterus obtained from a 3D ultrasound volume showing the
serosal fundus (labeled), the endometrial fundus (labeled) and the location of the two internal tubal
ostia (asterisks). Note that the indentation of the endometrial fundus (A) is measured as the distance
from a line connecting the two tubal ostia (dashed line) to the mid-endometrial fundus (arrow-A).
See Table 11.3 for details. Image is courtesy of Dr. Bernard Benoit.
Hình 11.21: Hình ảnh tử cung ở mặt phẳng giữa trán trên siêu âm 3D cho thấy thanh mạc vùng đáy
tử cung (Serosal fundus), nội mạc vùng đáy tử cung (Endometrial Fundus) và vị trí của 2 lỗ trong vòi
trứng (hoa thị). Lưu ý rằng chỗ lõm của nội mạc vùng đáy tử cung (A) được đo từ trung điểm đường
nối 2 lỗ trong vòi trứng đến điểm giữa nội mạc vùng đáy tử cung (mũi tên A). Xem thêm Bảng 11.3.
Hình ảnh do Dr. Bernard Benoit cung cấp.
We have described an easy technique for the retrieval of the midcoronal plane from a 3D uterine
volume (21). This standardized technique, termed, the Z-technique, is easy to learn, reduces
operator dependency and enhances the diagnostic accuracy of 3D ultrasound in the detection of
mullerian anomalies. Table 11.4 and corresponding Figures 11.22 to 11.26 details the sequence
of steps for the display of the midcoronal plane of the uterus from a 3D volume using the Ztechnique.
Chúng tôi đã mô tả một kỹ thuật đơn giản trong siêu âm 3D tử cung ở mặt phẳng giữa trán
(midcoronal plane) (21). Kỹ thuật này được gọi là kỹ thuật Z, dễ thực hiện, giảm thiểu sự phụ
thuộc vào người thực hiện và tăng độ chính xác trong chẩn đoán của siêu âm 3D trong việc
phát hiện các bất thường ống Muller. Bảng 11.4 tương ứng từ Hình 11.22 đến 11.26 cho thấy
các bước hiển thị tử cung ở mặt phẳng giữa trán từ siêu âm 3D sử dụng kỹ thuật Z.
TABLE 11.3 Classification of Mullerian Malformations by 3D Ultrasound
(Modified with Permission from Reference 20)


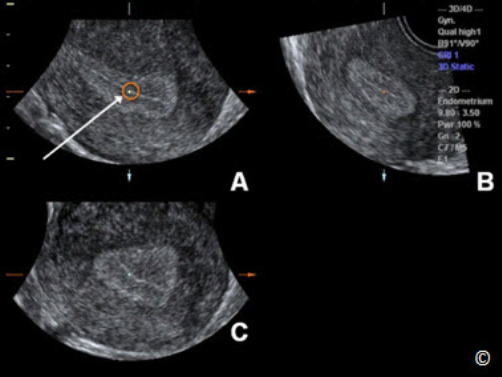
represents the reference plane (sagittal in this case) and B and C represent 2
orthogonal planes. The initial step in the Z-Technique involves placing the
reference/rotational point in the midlevel of the endometrial lining in plane
A (circle and arrow). Modified with permission from the American Institute
of Ultrasound in Medicine (21).
Hình 11.22: Hình ảnh tử cung ở nhiều mặt phẳng khác nhau trên siêu âm 3D.
Mặt phẳng A hiển thị mặt cắt tham chiếu (trường hợp này là mặt cắt dọc) và
các mặt phẳng B và C hiển thị 2 mặt cắt vuông góc. Bước đầu tiên trong kỹ
thuật Z là đặt điểm tham chiếu ở khoảng giữa của nội mạc tử cung trên mặt
phẳng A (vòng tròn và mũi tên).

Figure 11.23: 3D volume of the uterus (same as in Figure 11.22) in multiplanar display. The second step
in the Z-Technique involves aligning the long axis of the endometrial lining in plane A along the
horizontal axis (dashed arrows) by rotating plane A along the Z-axis (curved arrow). The white arrow
and circle shows the reference/rotational point. Modified with permission from the American Institute
of Ultrasound in Medicine (21).
Hình 11.23: Hình ảnh tử cung ở nhiều mặt phẳng khác nhau trên siêu âm 3D (tương tự Hình 11.22).
Bước thứ 2 trong kỹ thuật Z là chỉnh trục dọc của nội mạc tử cung nằm ngang ở mặt phẳng A (mũi tên
đứt đoạn) bằng cách xoay mặt phẳng A theo trục Z (mũi tên cong). Mũi tên trắng và vòng tròn thể hiện
điểm tham chiếu.

Figure 11.24: 3D volume of the uterus (same as in Figure 11.22) in multiplanar display. The third step
in the Z-Technique involves placing the reference/rotational point in the midlevel of the endometrial
lining in the transverse plane (plane B). The white arrow and circle shows the reference/rotational
point in B. Modified with permission from the American Institute of Ultrasound in Medicine (21).
Hình 11.24: Hình ảnh tử cung ở nhiều mặt phẳng khác nhau trên siêu âm 3D (tương tự Hình 11.22).
Bước thứ 3 trong kỹ thuật Z là đặt điểm tham chiếu ở khoảng giữa nội mạc tử cung trên mặt cắt
ngang (mặt phẳng B). Mũi tên trắng và vòng tròn thể hiện điểm tham chiếu ở mặt phẳng B.
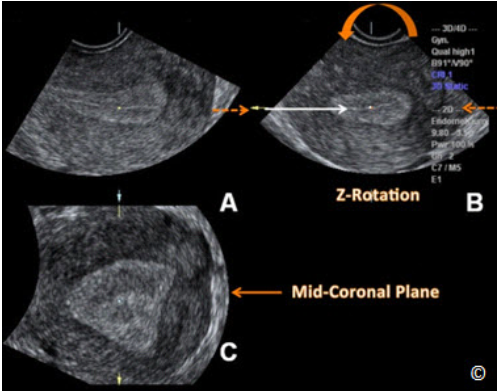
Figure 11.25: 3D volume of the uterus (same as in Figure 11.22) in multiplanar display. The fourth
step in the Z-Technique involves aligning the long axis of the endometrial lining in plane B along the
horizontal axis (dashed arrows) by rotating plane B along the Z-axis (curved arrow). Note that the
mid-coronal plane is displayed in plane C. The white arrow shows the reference/rotational point in
plane B. Modified with permission from the American Institute of Ultrasound in Medicine (21).
Hình 11.25: Hình ảnh tử cung ở nhiều mặt phẳng khác nhau trên siêu âm 3D (tương tự Hình 11.22).
Bước thứ 4 trong kỹ thuật Z là chỉnh trục dọc của nội mạc tử cung nằm ngang ở mặt phẳng B (mũi
tên đứt đoạn) bằng cách xoay mặt phẳng B theo trục Z (mũi tên cong). Lưu ý rằng mặt cắt giữa trán
(Mid-Coronal Plane) được hiển thị ở mặt phẳng C. Mũi tên trắng chỉ điểm tham chiếu ở mặt phẳng B.

Figure 11.26: 3D volume of the uterus (same as in Figure 11.22) in multiplanar display. The final step
(step 5) of the Z-technique involves applying Z rotation on plane C (curved arrow) to display the midcoronal plane in the traditional orientation. Modified with permission from the American Institute ofUltrasound in Medicine (21).
Hình 11.26: Hình ảnh tử cung ở nhiều mặt phẳng khác nhau trên siêu âm 3D (tương tự Hình 11.22).
Bước cuối cùng (bước 5) của kỹ thuật Z là dùng nút xoay Z trên mặt phẳng C để hiển thị mặt cắt giữa
trán theo hướng ‘truyền thống’. Hình ảnh được chỉnh sửa dưới sự cho phép của Viện Siêu âm Y khoa
Hoa Kỳ (21).
Several authors have reported on the high accuracy of 3D ultrasound when comparing it with
surgical findings in the diagnosis of uterine anomalies (22, 23). Furthermore, its accuracy
compared to MRI has been established (24). We recommend 3D ultrasound as the modality of
choice when evaluating a patient for a suspected uterine anomaly because of its relative low cost,
lack of ionizing radiation or iodine contrast agents and excellent diagnostic capability, in
addition to eliminating the need for laparoscopy in certain cases (25).
Nhiều tác giả báo cáo độ chính xác cao của siêu âm 3D khi so sánh với kết quả phẫu thuật
trong chẩn đoán bất thường tử cung (22,23), một vài nghiên cứu còn cho thấy độ chính xác
tương đương với MRI (24). Chúng tôi khuyến cáo sử dụng siêu âm 3D trên bệnh nhân có
nghi ngờ bất thường tử cung vì giá thành thấp, không có bức xạ ion, không sử dụng chất
tương phản và khả năng chẩn đoán vượt trội, tránh chỉ định nội soi ổ bụng không cần thiết
trong những trường hợp chắc chắn (25)
TABLE 11.4
The Z-Technique: Steps for the Retrieval of the Midcoronal Plane in a 3D
Volume of the Uterus [Modified with Permission from the American Institute
of Ultrasound in Medicine (21)].
Step 1. Place the reference/rotational point in the midlevel of the endometrial lining in the sagittal
plane (Figure 11.22)
Step 2. Use the Z rotation to align the long axis of the endometrial lining along the horizontal axis in
the sagittal plane of the uterus (Figure 11.23)
Step 3. Place the reference/rotational point in the midlevel of the endometrial lining in the
transverse plane (Figure 11.24)
Step 4. Use the Z rotation to align the endometrial lining with the horizontal axis in the transverse
plane of the uterus (Figure 11.25)
Step 5. After step 4, the midcoronal plane of the uterus will be displayed in plane C (Figure 11.25);
apply Z rotation on plane C to display the midcoronal plane in the traditional orientation (Figure
11.26).
BẢNG 11.4
Kỹ thuật Z: Các bước dựng lại hình ảnh tử cung ở mặt phẳng giữa trán
trên siêu âm 3D [Chỉnh sửa được Viện Siêu âm Y khoa Hoa Kỷ (21) chấp
nhận]
Bước 1. Đặt điểm tham chiếu/xoay ở khoảng giữa của lớp nội mạc tử cung trên mặt cắt dọc
(Hình 11.22)
Bước 2. Dùng nút xoay Z để chỉnh trục dọc của nội mạc tử cung nằm ngang ở mặt cắt dọc của
tử cung (Hình 11.23)
Bước 3. Đặt điểm tham chiếu/xoay ở khoảng giữa của lớp nội mạc tử cung ở mặt cắt ngang
(Hình 11.24)
Bước 4. Dùng nút xoay Z để chỉnh trục dọc của nội mạc tử cung nằm ngang ở mặt cắt ngang
của tử cung (Hình 11.25)
Bước 5. Sau bước 4, mặt cắt giữa trán của tử cung hiển thị ở mặt phẳng C (Hình 11.25), dùng
nút xoay Z trên mặt cắt C để hiển thị mặt cắt giữa trán theo hướng ‘truyền thống’ (Hình 11.26)
LEIOMYOMAS
U XƠ TỬ CUNG
Leiomyomas (fibroids) are the most common benign tumors encountered in gynecology as they
are seen in about 20 – 30 % of women older than 35 years of age (26). By 50 years of age, about
70% of white women and more than 80% of black women will have had at least one leiomyoma
with related significant symptoms in 15 to 30% of these women (26, 27). Histologically,
leiomyomas consist of smooth muscle with varying amount of connective tissue and their growth
is generally, estrogen dependent.
U xơ tử cung (Leiomyomas, Fibroids) là những khối u lành tính thường gặp nhất trong phụ
khoa chiếm khoảng 20 – 30% ở phụ nữ trên 35 tuổi (26). Ở độ tuổi 50, khoảng 70% phụ nữ
da trắng và hơn 80% phụ nữ da đen có ít nhất một u xơ tử cung và 15-30% trong số đó có
triệu chứng (26,27). Về mặt mô học, u xơ tử cung bao gồm cơ trơn và mô liên kết, sự phát
triển của u phụ thuộc vào estrogen.
The presence of leiomyosarcoma in a leiomyoma is rare and
occurs in about 0.2% of cases. Leiomyomas are more prevalent in black women (26) and despite
their estrogen dependency; only about 50 % show growth in association with pregnancy. In
postmenopausal women, leiomyomas typically regress in size and are rarely of clinical concern.
Sự hiện diện của sarcoma cơ tử cung (leiomyosarcoma)
trong u xơ tử cung hiếm gặp, chiếm khoảng 0,2% các trường hợp. U xơ tử cung gặp nhiều
hơn ở phụ nữ da đen (26), mặc dù u xơ tử cung phụ thuộc estrogen nhưng chỉ có khoảng 50%
khối u có tăng kích thước trong thai kỳ. Ở phụ nữ hậu mãn kinh, u xơ tử cung thường giảm
kích thước và hiếm khi gây triệu chứng lâm sàng.
Leiomyomas have pseudocapsules, which are formed of compressed surrounding myometrium.
Leiomyomas are usually multiple and most are asymptomatic and are discovered as palpable
masses, or uterine enlargement, on routine gynecologic examination. On occasions, they are
associated with abnormal uterine bleeding or pelvic pain.
U xơ tử cung có vỏ bao giả
(pseudocapsules) do sự chèn ép cơ tử cung xung quanh. U xơ tử cung thường nhiều u và hầu
hết không có triệu chứng, được phát hiện khi khám phụ khoa định kỳ sờ thấy khối u hoặc tử
cung to ra. Một số trường hợp, u xơ gây xuất huyết tử cung hoặc đau vùng chậu.
Leiomyomas arise from the uterine myometrium and can occupy various anatomic positions
within the uterus or surrounding structures. Table 11.5 lists various types of leiomyomas in
relation to their anatomic locations. The degree to which the leiomyoma projects into the
endometrial cavity is of clinical importance as it helps to determine whether the leiomyoma can
be resected hysteroscopically or not. In general, if the leiomyoma is protruding 50% or more into
the endometrial cavity, hysteroscopic resection can be achieved. Figure 11.27 is a schematic
over an ultrasound image of various types of leiomyomas and Figures 11.28 to 11.31 show
various types of leiomyomas on ultrasound.
U xơ tử cung xuất phát từ lớp cơ tử cung và có thể nằm ở các vị trí giải phẫu khác nhau trong
tử cung hoặc các cấu trúc xung quanh. Bảng 11.5 liệt kê các vị trí khác nhau của u xơ tử cung
về mặt giải phẫu. Mức độ phát triển của u xơ vào lòng tử cung có ý nghĩa lâm sàng quan
trọng giúp xác định khả năng cắt bỏ u xơ qua nội soi buồng tử cung. Thông thường, nếu u xơ
tử cung nhô vào lòng tử cung từ 50% trở lên thì có thể nội soi buồng tử cung để cắt u. Hình
11.27 là sơ đồ các loại u xơ tử cung và Hình 11.28 đến 11.31 cho thấy các loại u xơ tử cung
trên siêu âm.
TABLE 11.5 Anatomic Locations of Leiomyomas (Figure 11.27)
- Intramural: The leiomyoma is within the myometrium with minimal or no
bulging into the serosa or endometrium
- Subserosal: A significant portion of the leiomyoma is bulging into the serosal
surface
- Submucosal: A significant portion of the leiomyoma is bulging into the
endometrial cavity
- Pedunculated: The leiomyoma is exophytic and is attached to the uterus by a
pedicle
- Intracavitary: The leiomyoma is within the endometrial cavity and is attached to
the myometrium by a pedicle
- Parasitic: The leiomyoma is exophytic with blood supply obtained from an
adjacent structure other than the uterus
BẢNG11.5 Các Vị Trí Giải Phẫu Của U Xơ Tử Cung (Hình 11.27)
- Trong cơ (Intramural): U xơ nằm trong cơ không đội vào thanh mạc / nội mạc
tử cung hoặc đội ít
- Dưới thanh mạc (Subserosal): Phần lớn u xơ đội ra bề mặt thanh mạc
- Dưới niêm mạc (Submucosal): Phần lớn u xơ đội vào khoang nội mạc tử cung
- Có cuống (Pedunculated): U xơ nằm bên ngoài tử cung và có cuống dính vào tử
cung
- Trong lòng tử cung (Intracavitary): U xơ nằm trong buồng tử cung và có cuống
dính vào lớp cơ tử cung
- Cạnh tử cung (Parasitic): U xơ nằm bên ngoài tử cung được cấp máu chủ yếu từ
các cấu trúc lân cận tử cung

Figure 11.27: Transvaginal ultrasound of a midsagittal plane of the uterus with schematic overlay of
leiomyomas to describe their anatomic locations. 1 = Intracavitary, 2 = Submucosal with > 50% into
the endometrial cavity. 3 = Submucosal with < 50% into the endometrial cavity. 4 = Intramural. 5 =
Subserosal. 6 = Pedunculated. 7 = Parasitic.
Hình 11.27: Siêu âm qua ngã âm đạo, tử cung ở mặt cắt dọc giữa với sơ đồ hình vẽ để mô tả các vị
trí giải phẫu của u xơ tử cung. 1:trong lòng tử cung (intracavitary), 2:dưới niêm mạc (submucosal)
>50% nhô vào lòng tử cung, 3:dưới niêm mạc (submucosal) <50% nhô vào lòng tử cung, 4:trong cơ
(intramural), 5:dưới thanh mạc (subserosal), 6:có cuống (pedunculated), 7:cạnh tử cung (parasistic).
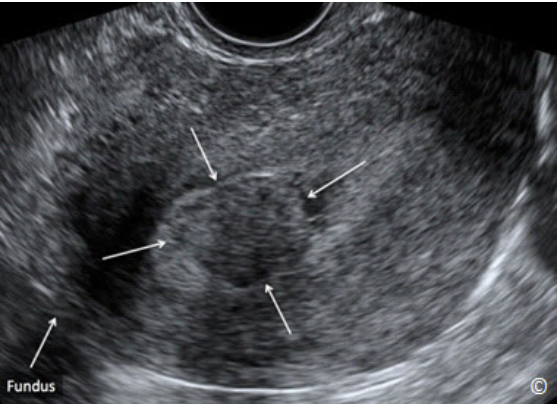
Figure 11.28: Transvaginal ultrasound of a midsagittal plane of the uterus showing a
submucosal (intracavitary) leiomyoma (arrows). Uterine fundus is labeled for image
orientation. See Table 11.6 for sonographic features. Image is courtesy of Dr. Bernard
Benoit.
Hình 11.28: Siêu âm tử cung qua ngã âm đạo ở mặt cắt dọc giữa cho thấy u xơ trong
lòng tử cung (intracavitary leiomyoma) (mũi tên). Đáy tử cung (Fundus) được gắn
nhãn để định hướng hình ảnh. Xem Bảng 11.6 về đặc điểm siêu âm.

Figure 11.29: Transvaginal ultrasound of a midsagittal plane of the uterus showing
an intramural leiomyoma (arrows). Uterine fundus is labeled for image orientation.
See Table 11.6 for sonographic features. Image is courtesy of Dr. Bernard Benoit.
Hình 11.29: Siêu âm tử cung qua ngã âm đạo ở mặt cắt dọc giữa cho thấy u xơ trong
cơ tử cung (intramural leiomyoma) (mũi tên). Đáy tử cung (Fundus) được gắn nhãn
để định hướng hình ảnh. Xem Bảng 11.6 về đặc điểm siêu âm.

Figure 11.30: Transvaginal ultrasound of a midsagittal plane of the uterus showing a
subserosal leiomyoma (arrows). Uterine fundus is labeled for image orientation. See
Table 11.6 for sonographic features. Image is courtesy of Dr. Bernard Benoit.
Hình 11.30: Siêu âm tử cung qua ngã âm đạo ở mặt cắt dọc giữa cho thấy u xơ dưới
thanh mạc (subserosal leiomyoma) (mũi tên). Đáy tử cung (Fundus) được gắn nhãn
để định hướng hình ảnh. Xem Bảng 11.6 về đặc điểm siêu âm

Figure 11.31: Transvaginal ultrasound of a midsagittal plane of the uterus showing a
pedunculated leiomyoma (arrows) in a posterior location to the uterus. Uterine
fundus is labeled for image orientation. See Table 11.6 for sonographic features.
Hình 11.31: Siêu âm tử cung qua ngã âm đạo ở mặt cắt dọc giữa cho thấy u xơ có
cuống (pendunculated leiomyoma) (mũi tên) ở thành sau tử cung. Xem Bảng 11.6
về đặc điểm siêu âm.
The sonographic features of leiomyomas are listed in Table 11.6 and the various types of
leiomyoma’s degeneration are listed in Table 11.7. Hyaline degeneration is the most common
and appears as anechoic areas within the central portion of a leiomyoma (Figure 11.32).
Đặc điểm siêu âm của u xơ tử cung được liệt kê trong Bảng 11.6 và các dạng thoái hóa của u
xơ tử cung được liệt kê trong Bảng 11.7. Thoái hóa Hyaline là thường gặp nhất và cho hình
ảnh một vùng echo trống ở trung tâm khối u xơ (Hình 11.32).
TABLE 11.6 Sonographic Features of Leiomyomas
- Solid echogenic mass arising from the uterine myometrium
- Well defined contour (pseudocapsule)
- Whorled appearance due to smooth muscle and connective tissue arranged in a
concentric pattern
- Significant attenuation of ultrasound beam
- Characteristic shadow pattern described as “venetian blind shadowing” (Figure
11.33)
- Minimal to moderate vascularity on color Doppler
- When pedunculated, the solid leiomyoma tends to move with the uterus and
distinctly from the ovary (Clip 11.1)
- Color Doppler can on occasions identify a stalk and connect it to the uterus in
pedunculated leiomyomas
BẢNG 11.6 Các Đặc Điểm Siêu Âm Của U Xơ Tử Cung
- Khối echo đặc xuất phát từ lớp cơ tử cung
- Giới hạn rõ (vỏ bao giả - pseudocapsule)
- Dạng xoắn ốc do cơ trơn và mô liên kết sắp xếp đồng tâm
- Làm suy giảm đáng kể chùm tia siêu âm
- Bóng lưng sọc vằn (venetain blind shadowing) (Hình 11.33)
- Tưới máu ít đến trung bình trên Doppler màu
- U xơ tử cung có cuống thường di chuyển cùng với tử cung và tách biệt với
buồng trứng (Clip 11.1)
- Trong một vài trường hợp u xơ tử cung có cuống, siêu âm Doppler màu giúp xác
định cuống nối với tử cung.

Figure 11.32: Transvaginal ultrasound showing a hyaline degeneration of an
intramural leiomyoma (labeled). The uterine fundus is labeled for image orientation.
Hình 11.32: Siêu âm qua ngã âm đạo, hình ảnh thoái hóa Hyaline của một u xơ tử
cung trong cơ (Degeneration). Đáy tử cung (Fundus) được gắn nhãn để định hướng
hình ảnh.

Hình 11.33: Siêu âm tử cung qua ngã âm đạo ở mặt cắt dọc giữa cho thấy u xơ tử
cung dưới thanh mạc (mũi tên). Lưu ý bóng lưng sọc vằn điển hình (venetain blinds
shadowing) (đường thẳng đứt đoạn). Đáy tử cung (Fundus) được gắn nhãn để định
hướng hình ảnh.
TABLE 11.7 Types of Leiomyoma Degeneration
- Atrophic
- Hyaline
- Carneous
- Myxoid
- Calcific
- Cystic
- Hemorrhagic
BẢNG 11.7 Các Dạng Thoái Hóa Của U Xơ Tử Cung
- Teo (Atrophic)
- Hyaline
- Thoái hóa đỏ (Red/Carneous)
- Dạng nhầy (Myxoid)
- Vôi hóa (Calcific)
- Dạng nang (Cystic)
- Xuất huyết (Hemorrhagic)
ENDOMETRIAL ABNORMALITIES
Abnormal Uterine Bleeding:
Abnormal uterine bleeding (AUB) is a term that describes abnormal menstrual flow in women of
reproductive age. AUB can be related to abnormal volume, duration, frequency and regularity of
menstrual flow. In an effort to standardize diagnosis and management of AUB, the International
Federation of Gynecology and Obstetrics (FIGO) in 2011, introduced a new classification of
AUB known by the acronym PALM-COEIN, which stands for polyps, adenomyosis, leiomyoma,
malignancy (hyperplasia), coagulopathy, ovulatory dysfunction, endometrial iatrogenic and not
yet classified (28).
Xuất huyết tử cung bất thường (Abnormal Uterine Bleeding - AUB) là một thuật ngữ mô tả
sự ra huyết âm đạo ngoài chu kỳ kinh có nguồn gốc từ tử cung ở phụ nữ trong độ tuổi sinh
sản. XHTCBT có lượng máu mất, thời gian, tần số và quy luật khác với chu kỳ kinh bình
thường. Để chuẩn hóa việc chẩn đoán và điều trị XHTCBT, Tổ chức Sản phụ khoa Quốc tế
(The International Federation of Gynecology and Obstetrics - FIGO) năm 2011 đã đưa ra một
phân loại mới của XHTCBT được viết tắt là PALM-COEIN đại diện cho polyps, adenomyosis (lạc nội mạc trong cơ tử cung), leiomyoma (u xơ tử cung), malignancy (bệnh ác
tính) (tăng sản nội mạc tử cung-hyperplasia), coagulopathy (rối loạn đông máu), ovulatory
dysfusion (rối loạn chức năng rụng trứng), endometrial iatrogenic (do điều trị) và not yet
classification (chưa phân loại được) (28).
The American Congress of Obstetrics and Gynecology (ACOG) supported
the adoption of this classification in the practice bulletin on diagnosis of AUB in reproductive
age women (29). The term dysfunctional uterine bleeding, which has been commonly used to
describe AUB, should be abandoned (28, 29).
Hiệp hội Sản phụ khoa Hoa Kỳ (ACOG) đã ủng hộ
áp dụng phân loại này trên tạp chí thực hành chẩn đoán XHTCBT ở phụ nữ trong độ tuổi sinh
sản (29). Thuật ngữ XHTCBT do rối loạn chức năng (dysfunctional uterine bleeding) thường
dùng để chỉ xuất huyết tử cung bất thường nên bỏ đi (28,29).
The evaluation of women with AUB is beyond the scope of this textbook, but in general should
include a history, physical examination, laboratory and imaging studies and endometrial
sampling when indicated, based upon the age of symptomatic women. There is insufficient
evidence to recommend the use of transvaginal ultrasound for endometrial thickness evaluation
in AUB in women of reproductive age unless there are risk factors for endometrial carcinoma.
Việc đánh giá bệnh nhân XHTCBT nằm ngoài phạm vi của sách này nhưng thông thường bao
gồm bệnh sử, khám lâm sàng, các xét nghiệm và hình ảnh học, sinh thiết nội mạc tử cung nếu
có chỉ định, tùy thuộc vào độ tuổi của bệnh nhân có triệu chứng. Không đủ bằng chứng để
khuyến cáo sử dụng siêu âm qua ngã âm đạo để đánh giá nội mạc tử cung dày ở phụ nữ
XHTCBT trong độ tuổi sinh sản nếu không có các yếu tố nguy cơ của ung thư nội mạc tử
cung (endometrial carcinoma).
Transvaginal ultrasonography is useful however as a screening test to assess the endometrial
cavity for leiomyomas and polyps. In postmenopausal women, transvaginal ultrasound has the
ability to exclude malignancy when the endometrial lining is uniform and is 4 mm or less. This is
discussed in more details later in this chapter.
Siêu âm qua ngã âm đạo được dùng như một phương pháp
sàng lọc giúp đánh giá lòng tử cung để phát hiện u xơ tử cung và polyp. Ở phụ nữ mãn kinh,
siêu âm qua ngã âm đạo cho thấy nội mạc tử cung đồng dạng và mỏng từ 4mm trở xuống
giúp loại trừ khả năng ác tính. Điều này sẽ được bàn sâu trong chương này
Endometrial Polyps and Submucosal Leiomyomas:
Polyp Nội Mạc Và U Xơ Tử Cung Dưới Niêm
Common focal intracavitary endometrial lesions include polyps and submucosal leiomyomas as
they account for 30% and 10% of causes of postmenopausal bleeding respectively (30).
Sonohysterography has been shown to be a superior imaging modality in the evaluation of
intracavitary endometrial lesions such as polyps (Figure 11.34) and leiomyomas, when
compared to transvaginal ultrasound alone (31). The efficacy of sonohysterography in the
diagnosis of endometrial polyps and submucosal leiomyomas has been shown to be equal to
hysteroscopy in some series (32).
Tổn thương khu trú nội mạc tử cung thường gặp bao gồm polyp nội mạc và u xơ tử cung dưới
niêm lần lượt chiếm khoảng 30% và 10% các trường hợp xuất huyết hậu mãn kinh (3). Siêu
âm bơm nước buồng tử cung là một phương pháp chẩn đoán hình ảnh vượt trội so với siêu
âm ngã âm đạo đơn thuần trong việc đánh giá các tổn thương nội mạc lòng tử cung như polyp
(Hình 11.34) và u xơ tử cung (31). Hiệu quả của siêu âm bơm nước buồng tử cung trong
chẩn đoán polyp nội mạc và u xơ tử cung dưới niêm đã được chứng minh tương đương với
nội soi buồng tử cung trong nhiều nghiên cứu (32).

Figure 11.34: Transvaginal sonohysterography with color Doppler of a midsagittal plane of
the uterus showing an endometrial polyp (asterisk). Note the increased echogenicity of the
polyp as compared to myometrial tissue.
Hình 11.34: Siêu âm bơm nước buồng tử cung qua ngã âm đạo với Doppler màu ở mặt cắt
dọc giữa tử cung cho thấy một polyp nội mạc tử cung (dấu hoa thị). Lưu ý hồi âm của polyp
cao hơn mô cơ tử cung.
Endometrial polyps appear on sonohysterography as more echogenic than the surrounding
myometrium, completely contained within the endometrial cavity with no extension into the
myometrium, homogeneous in echo texture with a narrow base of attachment to the underlying
myometrium (Figure 11.34). Color Doppler may demonstrate a vascular pedicle at the base of
the polyp in most cases (Figure 11.35 and 11.36). Cystic changes within a polyp are
occasionally seen and polyps can also be seen in the isthmic portion of the cavity (Figure 11.36)
and endocervical canal.
Polyp nội mạc tử cung trên siêu âm bơm nước buồng tử cung có hồi âm cao hơn cơ tử cung
xung quanh, nằm hoàn toàn trong buồng tử cung không lấn vào lớp cơ, có hồi âm đồng nhất
với phần đáy hẹp dính với cơ tử cung (Hình 11.34). Siêu âm Doppler màu giúp xác định một
cuống mạch máu nằm ở phần đáy của polyp trong đa số các trường hợp (Hình 11.35 và
11.36). Đôi khi có những biến đổi dạng nang bên trong polyp. Polyp cũng có thể xuất hiện ở
đoạn eo của khoang nội mạc (Hình 11.36) và kênh cổ tử cung.
Submucosal leiomyomas appear on sonohysterography as less echogenic
than the surrounding endometrium, broad-based and lift the surrounding endometrium as they
project to varying degrees into the cavity (Figure 11.37). Given that submucosal leiomyomas
arise from the subendometrial myometrium, a portion of the leiomyoma extends into the
myometrium: a differentiating feature from an endometrial polyp. Submucosal leiomyomas tend
to shadow the ultrasound beam, another important distinctive feature from endometrial polyps
(Figure 11.37). Table 11.8 lists differentiating features of polyps and submucosal leiomyomas.
The degree to which the submucosal leiomyoma projects into the endometrial cavity is of clinical
relevance. Extension of a leiomyoma by more than 50% of its surface into the cavity allows for
possible hysteroscopic resection.
U xơ tử cung dưới niêm mạc
trên siêu âm bơm nước buồng tử cung có hồi âm thấp hơn cơ tử cung xung quanh, đáy rộng
và đội nội mạc tử cung khi chúng phát triển vào khoang nội mạc với các mức độ khác nhau
(Hình 11.37). U xơ tử cung dưới niêm mạc xuất phát từ lớp cơ tử cung dưới niêm mạc nên
một phần u xơ tử cung kéo dài đến lớp cơ tử cung, đây là một đặc điểm phân biệt với polyp
nội mạc tử cung. Một đặc điểm quan trọng khác để phân biệt với polyp nội mạc là u xơ tử
cung dưới niêm thường có bóng lưng trên siêu âm (Hình 11.37). Bảng 11.8 liệt kê các đặc
điểm phân biệt giữa polyp và u xơ dưới niêm. Mức độ phát triển của u xơ dưới niêm vào lòng
tử cung có liên quan với lâm sàng. U xơ tử cung đội vào khoang nội mạc trên 50% cho phép
nội soi buồng tử cung cắt u.

Figure 11.35: Transvaginal ultrasound with color Doppler of a midsagittal plane of the
uterus showing a small endometrial polyp (arrows). Note the increased echogenicity of the
polyp as compared to myometrial tissue and a vascular pedicle noted on color Doppler.
The uterine fundus is labeled for image orientation.
Hình 11.35: Siêu âm qua ngã âm đạo với Doppler màu ở mặt cắt dọc giữa tử cung cho thấy
một polyp nội mạc tử cung nhỏ (mũi tên). Lưu ý hồi âm của polyp cao hơn so với cơ tử
cung và sự hiện diện của cuống mạch máu ( Vascular Pedicile) trên Doppler màu. Đáy tử
cung (Fundus) được dán nhãn để định hướng hình ảnh.

Figure 11.36: Transvaginal ultrasound with color Doppler of a midsagittal plane of the uterus
showing an endometrial polyp (asterisk) in the isthmic portion of the endometrial cavity.
Note the presence of a vascular pedicle on color Doppler. The uterine fundus is labeled for
image orientation.
Hình 11.36: Siêu âm qua ngã âm đạo với Doppler màu ở mặt cắt dọc giữa tử cung cho thấy
một polyp nội mạc tử cung (dấu hoa thị) ở đoạn eo của khoang nội mạc. Lưu ý sự hiện diện
của cuốn mạch máu trên Doppler màu. Đáy tử cung (Fundus) được gắn nhãn để định hướng
hình ảnh

Figure 11.37: Transvaginal sonohysterography of a midsagittal plane of the uterus
showing a submucosal leiomyoma (asterisk). Note that the echogenicity of the leiomyoma
is comparable to that of the myometrium. The lifted endometrium (labeled – equal sign) is
noted surrounding the leiomyoma in the endometrial cavity. Also note the shadowing
(shadow – dashed lines) from the leiomyoma. The uterine fundus is labeled for image
orientation. Image is courtesy of Dr. Bernard Benoit.
Hình 11.37: Siêu âm qua ngã âm đạo với Doppler màu ở mặt cắt dọc giữa tử cung cho
thấy một u xơ tử cung dưới niêm mạc (dấu hoa thị). Lưu ý hồi âm của u xơ tử cung dưới
niêm tương đượng với cơ tử cung. Nội mạc tử cung bị đội lên (dấu bằng) bao quanh u xơ
trong khoang nội mạc. Chú ý bóng lưng (shadow-mũi tên đứt đoạn) của u xơ tử cung. Đáy
tử cung (Fundus) được gắn nhãn để định hướng hình ảnh.
TABLE 11.8
Differentiating Sonographic Features of Endometrial Polyps and Submucosal
Leiomyomas
- Polyp are contained within the endometrial cavity whereas Leiomyomas extend into the
myometrium
- Echogenicity of polyps is similar to endometrial lining whereas echogenicity of leiomyomas is
similar to myometrium (less)
- Polyps tend to have a visible vascular pedicle on color Doppler and are homogeneous in
echotexture
- Leiomyomas lift the endometrial lining
- Leiomyomas tend to shadow the ultrasound beam
BẢNG 11.8 Các đặc điểm siêu âm giúp phân biệt Polyp nội mạc tử cung và u xơ tử cung
dưới niêm mạc
- Polyp nằm hoàn toàn trong khoang nội mạc tử cung trong khi u xơ tử cung kéo dài đến lớp cơ
tử cung
- Độ hồi âm của polyp tương tự lớp nội mạc tử cung trong khi độ hồi âm của u xơ tử cung tương
tự cơ tử cung (kém hơn)
- Polyp thường có một cuống mạch máu nhìn thấy được trên Doppler màu và cấu trúc echo đồng
nhất
- U xơ tử cung đội vào lớp nội mạc tử cung
- U xơ tử cung thường có bóng lưng
Endometrial Adhesions and Retained Products of Conception:
Dính Lòng Tử Cung Và Sót Thai Sót Nhau
Other endometrial pathology amenable to diagnosis by sonohysterography includes intrauterine
adhesions, and retained products of conception. Intrauterine adhesions are clearly visible on
sonohysterography as thick or thin echogenic bands that attach to the endometrial walls (Figure
11.38). Sonohysterography is the best imaging modality for the detection of intrauterine
adhesions (33) and should be considered in patients with prior intrauterine instrumentation.
Retained products of conception appear as an echogenic mass within the endometrial cavity
(Figure 11.39). They are typically seen in women following an abortion, a miscarriage or a
delivery.
Một số bệnh lý khác của nội mạc có thể chẩn đoán bằng siêu âm bơm nước buồng tử cung
bao gồm dính lòng tử cung (intrauterine adhesions) và sót thai sót nhau (retained products of
conception-RPOC). Dính lòng tử cung thấy rõ trên siêu âm bơm nước buồng tử cung như một
dải echo dày (kích thước dày hoặc mỏng) bám vào thành nội mạc (Hình 11.38). Siêu âm bơm
nước buồng tử cung là phương tiện hình ảnh tốt nhất để chẩn đoán dính lòng tử cung (33)
được cân nhắc ở những bệnh nhân có can thiệp dụng cụ vào buồng tử cung trước đó. Sót thai
sót nhau có hình ảnh là một khối echo dày trong lòng tử cung (Hình 11.39). Thường gặp ở
những phụ nữ sau phá thai, sẩy thai hoặc sau sanh.

Figure 11.38: Transvaginal sonohysterography in a patient with suspected endometrial
adhesions. Note the presence of a thin reflective membrane in the sagittal (arrow in A) and
coronal (arrow in B) plane. These planes were obtained from a 3D volume.
Hình 11.38: Siêu âm bơm nước buồng tử cung ở một bệnh nhân nghi ngờ có dính buồng tử
cung. Lưu ý sự hiện diện của lớp màng mỏng trong mặt phẳng dọc (mũi tên A) và ngang (mũi
tên B). Các mặt phẳng này có được từ siêu âm 3D thể tích.
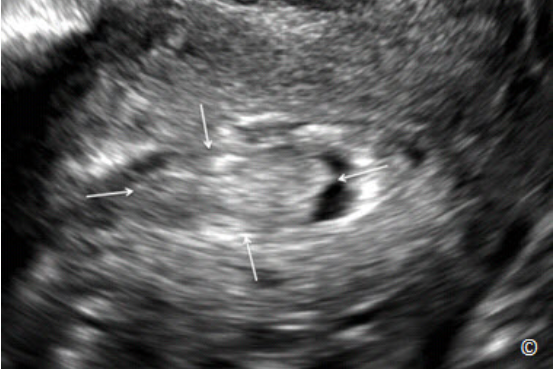
Figure 11.39: Transvaginal sonohysterography of the uterus in sagittal plane showing an echogenic mass (arrows) suggestive of retained products of conception.
Hình 11.39: Siêu âm bơm nước buồng tử cung ở mặt phẳng dọc giữa cho thấy một
khối echo dày (mũi tên) nghi ngờ sót thai hoặc sót nhau. Bệnh nhân này sanh khó 5
tuần trước.
Endometrial Hyperplasia and Cancer:
Tăng Sản Nội Mạc Tử Cung Và Ung Thư
Endometrial cancer is the most common gynecologic cancer in the United States, with vaginal
bleeding being the most common presenting symptom (34, 35). When postmenopausal women
present with vaginal bleeding, a systemic approach should be performed to rule-out endometrial
cancer or hyperplasia. An endometrial thickness that is 4 mm or less on a transvaginal ultrasound
in women presenting with postmenopausal bleeding, practically excludes endometrial cancer and
further endometrial evaluation is not warranted. Transvaginal ultrasound is therefore a
reasonable first approach to the evaluation and management of postmenopausal bleeding.
Ung thư nội mạc tử cung (endometrial cancer) là loại ung thư phụ khoa thường gặp nhất ở
Mỹ với triệu chứng thường gặp nhất là xuất huyết âm đạo (34,35). Khi phụ nữ mãn kinh có
xuất huyết âm đạo, cần tiếp cận một cách hệ thống để lọai trừ ung thư nội mạc tử cung và
tăng sản nội mạc tử cung (hyperplasia). Nếu nội mạc tử cung dày từ 4mm trở xuống trên siêu
âm qua ngã âm đạo ở phụ nữ xuất huyết hậu mãn kinh có thể giúp loại trừ ung thư nội mạc tử
cung và không cần tiến hành các phương pháp đánh giá nội mạc sâu hơn. Do đó, siêu âm qua
ngã âm đạo là phương pháp tiếp cận đầu tiên để đánh giá và theo dõi chảy máu sau mãn kinh.
If the
endometrial thickness is greater than 4 mm, further evaluation is needed with endometrial
sampling, sonohysterography or hysteroscopy. If endometrial sampling has been performed first
and insufficient tissue was obtained for diagnosis, a transvaginal ultrasound can be performed
and if it shows an endometrial thickness of 4 mm or less, no further evaluation is needed (36).
The significance of an endometrial thickness of greater than 4 mm in asymptomatic women is
unclear and should not prompt further work-up unless the patient is at a significantly increased
risk for endometrial cancer (37).
Nếu nội mạc tử cung dày trên 4mm, cần thực hiện những phương pháp đánh giá nội mạc tử
cung sâu hơn bao gồm: sinh thiết nội mạc, siêu âm bơm nước buồng tử cung và nội soi buồng
tử cung. Nếu sinh thiết nội mạc được thực hiện đầu tiên nhưng mẫu mô không đủ để chẩn
đoán thì có thể kết hợp siêu âm qua ngã âm đạo và nếu nội mạc tử cung dày < 4mm thì không
cần đánh giá thêm (36). Nội mạc tử cung dày > 4mm ở phụ nữ không triệu chứng không có ý
nghĩa rõ ràng và không nên làm gì thêm nếu bệnh nhân không nằm trong nhóm nguy cơ cao
ung thư nội mạc tử cung (37)
It is important to note that endometrial thickness should only be
measured when a midsagittal plane of the uterus is obtained with clear depiction of the
endometrial thickness from the fundal to the uterine isthmic / cervical area (Figure 11.13). If
such a plane cannot be obtained, or visualization of the endometrial thickness is unclear,
This patient had a complicated delivery 5 weeks prior.
transvaginal ultrasound cannot be used in the evaluation of women with postmenopausal
bleeding and alternate methods should be obtained. The validity of transvaginal ultrasound as a
screening tool for endometrial cancer has not been established and thus it should not be used for
this clinical indication.
Điều quan trọng cần lưu ý là chỉ nên đo độ dày nội mạc ở mặt
phẳng dọc giữa tử cung (midsagital plane) với nội mạc từ vùng đáy đến vùng thân/cổ tử cung
được quan sát rõ (Hình 11.13). Nếu không cắt được mặt phẳng này hoặc không thể quan sát
rõ bề dày của nội mạc tử cung thì siêu âm qua ngã âm đạo không được dùng để đánh giá nội
mạc ở phụ nữ xuất huyết hậu mãn kinh và phải thay thế bằng phương pháp khác. Giá trị của
việc sử dụng siêu âm qua ngã âm đạo như một phương pháp sàng lọc ung thư nội mạc tử
cung chưa được chứng minh vì vậy không nên áp dụng trên lâm sàng.
Endometrial hyperplasia can be diffuse or focal. Diffuse endometrial hyperplasia will appear on
sonohysterography as thickening of the endometrium. Focal endometrial hyperplasia on the other
hand is seen as a broad-based echogenic mass that does not distort the endometrial-myometrial
junction. Differentiating focal endometrial hyperplasia from an endometrial polyp can at times
be difficult. Endometrial cancer has similar sonographic characteristics to endometrial
hyperplasia or an enlarged polyp, with the exception of myometrial invasion, which can be
occasionally visible on ultrasound. Figures 11.40 to 11.42 represent transvaginal ultrasounds of
endometrial and uterine cancers.
Tăng sản nội mạc tử cung (Hyperplasia) có thể lan tỏa hoặc khu trú. Trên siêu âm bơm nước
buồng tử cung, tăng sản nội mạc lan tỏa biểu hiện là sự dày lên của nội mạc tử cung. Trong
khi đó tăng sản nội mạc tử cung khu trú biểu hiện là một khối echo dày có đáy rộng nhưng
không gây biến dạng vùng chuyển tiếp nội mạc-cơ tử cung. Đôi khi khó hẩn đoán phân biệt
giữa tăng sản nội mạc tử cung khu trú và polyp nội mạc tử cung. Ung thư nội mạc tử cung có
các đặc điểm siêu âm tương tự tăng sản nội mạc tử cung hoặc một polyp lớn, tuy nhiên ung
thư có xâm lấn cơ tử cung và một số trường hợp có thể nhìn thấy trên siêu âm. Hình 11.40
đến 11.42 cho thấy hình ảnh siêu âm của ung thư nội mạc và tử cung.

Figure 11.40: Transvaginal ultrasound of a sagittal plane of the uterus in a woman with
endometrial cancer. Note the enlarged, heterogeneous and thickened endometrium
(arrows).
Hình 11.40: Siêu âm tử cung qua ngã âm đạo tử cung với mặt phẳng đứng dọc ở bệnh
nhân ung thư nội mạc tử cung. Lưu ý nội mạc tử cung dày và không đồng nhất (mũi
tên).

Figure 11.41: Transvaginal sonohysterography of a sagittal plane of the uterus in
a woman with endometrial cancer. Note the multiple papillary projections
(arrows) in the endometrial cavity.
Hình 11.41: Siêu âm bơm nước buồng tử cung với mặt phẳng đứng dọc ở bệnh
nhân ung thư nội mạc tử cung. Lưu ý có nhiều chồi trong khoang nội mạc tử
cung (mũi tên)

Figure 11.42: Transvaginal ultrasound of a parasagittal plane of the uterus in a
patient presenting with a uterine mass. Note the presence of a complex mass
(arrows), which was a uterine stromal sarcoma on pathologic evaluation.
Hình 11.42: Siêu âm bơm nước buồng tử cung với mặt phẳng đứng dọc ở bệnh
nhân có khối u tử cung. Lưu ý bệnh học của khối hỗn hợp (mũi tên) là sarcoma tử
cung
Arteriovenous Malformations:
Dị Dạng Động Tĩnh Mạch
Uterine arteriovenous malformations (AVM) are rare and represent direct communications
between the arterial and venous system. They typically arise following instrumentation of the
endometrial cavity, commonly in association with pregnancy loss or delivery. On occasions, they
are associated with malignancies, infections or retained products of conception in molar
pregnancies (38, 39). AVM can also be congenital in nature and as such, they are less common
and symptomatic than the acquired variety (40).
Dị dạng động tĩnh mạch tử cung (AVM-ateriovenous malformations) khi có sự thông nối trực
tiếp giữa hệ thống động mạch và tĩnh mạch tử cung và là một bất thường hiếm gặp. Thường
xảy ra sau các can thiệp dụng cụ vào buồng tử cung (hay gặp trong sẩy thai hoặc sanh non).
Đôi khi, chúng có liên quan đến bệnh lý ác tính, nhiễm trùng hoặc sót thai sót nhau trong thai
trứng (38,39). AVM cũng có thể bẩm sinh, dạng nảy ít gặp hơn và ít triệu chứng hơn dạng
mắc phải (40).
The most common clinical presentation of AVM is heavy vaginal bleeding in patients who had
instrumentation of the endometrial cavity following a pregnancy. Other less common symptoms
include pelvic pain and dyspareunia. The diagnosis of AVM is best achieved by a transvaginal
ultrasound with color and pulsed Doppler. On grey scale ultrasound, AVM are seen as anechoic
spaces within the uterus, with irregular contour, typically located within the myometrium near its
junction with the endometrium (Figure 11.43).
Biểu hiện lâm sàng thường gặp của AVM là xuất huyết âm đạo nhiều ở bệnh nhân có can
thiệp dụng cụ vào buồng tử cung sau khi mang thai. Các triệu chứng khác ít gặp hơn bao gồm
đau vùng chậu (pelvic pain) và đau khi giao hợp (dyspareunia). Chẩn đoán AVM tốt nhất qua
siêu âm ngã âm đạo với Doppler màu hoặc Doppler xung. Trên siêu âm thang xám, AVM là
những vùng phản âm trống (anechoic), bờ không đều, thường nằm trong cơ tử cung gần vùng
chuyển tiếp với nội mạc tử cung (Hình 11.43).
Color Doppler shows turbulent flow within the
anechoic spaces with aliasing (Figure 11.44), and pulsed Doppler demonstrates high-velocity,
low impedance flow patterns (Figure 11.45). Color and pulsed Doppler is helpful in confirming
the presence of AVM and also in differentiating AVM from pseudoaneurysms. Pseudoaneuryms,
which can also occur following instrumentation of the uterine cavity, have swirling arterial blood
in them with high-velocity and high impedance blood flow patterns on color and pulsed Doppler
evaluation (41).
Trên siêu âm Doppler màu cho hình ảnh dòng
chảy xoáy (turbulent flow) bên trong những vùng phản âm trống (Hình 11.44) và Doppler
xung cho thấy dòng chảy có vận tốc cao, trở kháng thấp (Figure 11.45). Siêu âm Doppler
màu và Doppler xung hữu ích trong việc chẩn đoán AVM và giúp phân biệt với giả phình
mạch (pseudoaneurysm). Giả phình mạch cũng có thể xuất hiện sau can thiệp dụng cụ vào
buồng tử cung, có dòng máu xoáy bên trong động mạch, có vận tốc cao và trở kháng cao trên
siêu âm Doppler màu và Doppler xung (41).
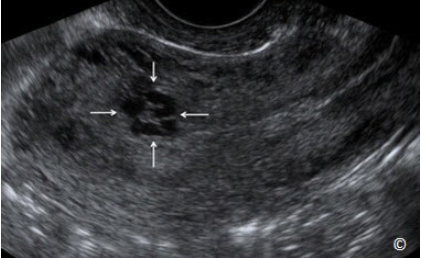
Figure 11.43: Transvaginal ultrasound of a sagittal plane of the uterus showing an arteriovenous malformation (AVM) (arrows). Note the sonographic appearance of AVM as
anechoic spaces, with irregular contour, located within the myometrium near its junction
with the endometrium.
Hình 11.43: Siêu âm qua ngã âm đạo ở mặt cắt dọc tử cung cho thấy dị dạng động tĩnh
mạch (AVM-ateriovenous malformations) (mũi tên). Lưu ý hình ảnh siêu âm của AVM là
những vùng echo trống có bờ không đều nằm trong cơ tử cung gần vùng chuyển tiếp với nội
mạc tử cung

Figure 11.44: Transvaginal ultrasound with color Doppler of a sagittal plane of the uterus
showing the same arterio-venous malformation (AVM) (arrows) as that in Figure 11.43.
Note the presence of blood flow within the AVM with turbulence and aliasing.
Hình 11.44: Siêu âm Doppler màu qua ngã âm đạo ở mặt cắt dọc tử cung dị dạng động
tĩnh mạch ở Hình 11.43 (mũi tên). Lưu ý sự hiện diện của dòng máu xoáy bên trong AVM.

Figure 11.45: Transvaginal ultrasound with color and pulsed Doppler of a sagittal plane of
the uterus showing the same arterio-venous malformation (AVM) (arrows) as that in figure
11.43. Note the pulsed Doppler waveforms showing low-impedance, high velocity (100
cm/sec) flow.
Hình 11.45: Siêu âm qua ngã âm đạo phổ Doppler màu và Doppler xung ở mặt cắt dọc tử
cung dị dạng động tĩnh mạch ở Hình 11.43 (mũi tên). Lưu ý dạng sóng dòng chảy có trở
kháng thấp, vận tốc cao (100 cm/giây).
Management of AVM should include a conservative approach following diagnosis, assuming
that the bleeding is not very heavy and the patient is not significantly anemic. Our experience
and that of others suggest resolution of AVM in a significant number of women with
conservative management over a 2-5 months period (42). Transcatheter arterial embolization is
the preferred method of treatment if conservative management fails, or bleeding is very heavy.
Transcatheter arterial embolization has a reported success rate of 50 – 70 % (43). Long-term
prognosis is good for women with AVM that regressed following conservative management or
with arterial embolization with reports of successful pregnancies (44).
AVM nên được điều trị bảo tồn nếu bệnh nhân không ra máu nhiều và tình trạng thiếu máu
không đáng kể. Theo kinh nghiệm của chúng tôi và một số chuyên gia khác đề nghị điều trị
bảo tồn bệnh nhân có AVM với thời gian từ 2 – 5 tháng (42). Thuyên tắc động mạch qua
catheter là phương pháp được ưa chuộng nếu điều trị bảo tồn thất bại hoặc trong trường hợp
ra máu nhiều. Thuyên tắc động mạch qua catheter được báo cáo thành công với tỷ lệ 50 –
70% (43). Tiên lượng lâu dài tốt (khả năng có thai) ở những phụ nữ AVM thoái triển sau điều
trị bảo tồn hoặc thuyên tắc động mạch (44).
CLIP 11.1

References:
1) AIUM practice guideline for the performance of pelvic ultrasound examinations.
American Institute of Ultrasound in Medicine. J Ultrasound Med. 2010; 29 (1):166-72.
2) AIUM practice guideline for ultrasonography in reproductive medicine. American
Institute of Ultrasound in Medicine; Society for Reproductive Endocrinology and
Infertility; American Society of Reproductive Medicine. J Ultrasound Med.
2009;28(1):128-37.
3) Bonnamy L, Marret H, Perrotin F, Body G, Berger C, Lansac J. Sonohysterography: a
prospective survey of results and complications in 81 patients. Eur J Obstet Gynecol
Reprod Biol 2002;102:42-47.
4) Merz E, Miric-Tesanic D, Bahlmann F, Weber G, Wellek S. Sonographic size of uterus
and ovaries in pre- and postmenopausal women. Ultrasound Obstet Gynecol.
1996;7(1):38-42.
5) Fleischer AC, Kalemeris GC, Entman SS. Sonographic depiction of the endometrium
during normal cycles. Ultrasound Med Biol. 1986;12(4):271-7.
6) Santolaya-Forgas J. Physiology of the menstrual cycle by ultrasonography. J Ultrasound
Med. 1992;11(4):139-42.
7) Duijkers IJ, Klipping C. Ultrasonographic assessment of endocervix and cervical mucus
in ovulatory menstrual cycles. Eur J Obstet Gynecol Reprod Biol. 2000;93(1):13-7.
8) R Azziz. Adenomyosis: current perspectives. Obstet Gynecol Clin North Am
1989;16:221-35.
9) Sakhel K, Abuhamad A. Sonography of Adenomyosis. J Ultrasound Med 2012
May;31(5):805-8.
10) Botsis D, Kassanos D, Antoniou G, Pyrgiotis E, Karakitsos P, Kalogirou D.
Adenomyoma and leiomyoma: differential diagnosis with transvaginal sonography. J
Clin Ultrasound. 1998;26(1):21-5.
11) Chiang CH, Chang MY, Hsu JJ. Tumor vascular pattern and blood flow impedance in the
differential diagnosis of leiomyoma and adenomyosis by color Doppler sonography. J
Assist Reprod Genet. 1999;16(5):268-75.
12) Acien P, Acien M, Sanchez-Ferrer ML. Complex malformations of the female genital
tract. New types and revision of classification. Hum Reprod 2004; 19:2377-2384
13) Raga F, Bauset C, Remohi J, Bonilla-Musoles F, Simon C, Pellicer A. Reproductive
impact of congenital Mullerian anomalies. Hum Reprod 1997;12(10):2277-2281
14) Rock JA and Schlaff WD. The obstetric consequences of uterovaginal anomalies. Fertil
Steril 1985; 43:681
15) Ludmir J, Samuels P, Brooks S. Pregnancy outcome of patients with uncorrected uterine
anomalies managed in a high risk obstetric setting. Obstet Gynecol 1990; 75:906
16) The American Fertility Society. The American Fertility Society classifications on adnexal
adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubalChapter 11: Ultrasound of the Non-Pregnant Uterus 251
pregnancies, Mullerian anomalies and intrauterine adhesions. Fertil Steril 1988;49:944-
955.
17) Pellerito JS,McCarthy SM, Doyle MB, Glickman MG, DeCherney AH. Diagnosis of
uterine anomalies: relative accuracy of MR imaging, endovaginal ultrasound, and
hysterosalpingography. Radiology 1992; 183:795-800.
18) Bocca SM, Abuhamad AZ. Use of 3-dimensional sonography to assess uterine anomalies.
J Ultrasound in Medicine 2013;32:1.
19) Randolph J, Ying Y, Maier D, Schmidt C, Riddick D. Comparison of real time
ultrasonography, hysterosalpingography, and laparoscopy/hysteroscopy in the evaluation
of uterine abnormalities and tubal patency. Fertil Steril 1986; 5:828-832.
20) Salim R, Woelfer B, Backos M, Regan L, Jurkovic D. Reproducibility of threedimensional ultrasound diagnosis of congenital uterine anomalies. Ultrasound Obstet
Gynecol 2003; 21:578–582.
21) Abuhamad A, Singleton S, Zhao Y, Bocca S. The Z technique: an easy approach to the
display of the mid-coronal plane of the uterus in volume sonography. J Ultrasound Med
2006; 25:607-612.
22) Deutch T, Bocca S, Oehninger S, et al. Magnetic resonance imaging versus threedimensional transvaginal ultrasound for the diagnosis of Mullerian anomalies. Fertil
Steril 2006;86:S308
23) Bocca S, Abuhamad A. Use of 3-Dimensional Sonography to Assess Uterine
Anomalies. J Ultrasound Med 2013;32:1-6.
24) Deutch TD, Abuhamad AZ. The role of 3-dimensional ultrasonography and magnetic
resonance imaging tin the diagnosis of mullerian duct anomalies: a review of the
literature. J Ultrasound Med 2008;27(3):413-23.
25) Bocca SM, Oehninger S, Stadtmauer L, Agard J, Duran H, Sarhan A, Horton S,
Abuhamad A. Prospective study to evaluate the costs, accuracy, risks and benefits of 3D
ultrasound compared to other imaging modalities in women with intrauterine lesions. J
Ultrasound Med 2012;31:81-85.
26) Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence
of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet
Gynecol 2003;188:100-7.
27) Catherino WH, Parrott E, Segars J. Proceedings from the National Institute of Child
Health and Human Development conference on the Uterine Fibroid Research Update
Workshop. Fertil Steril 2011;95:9-12
28) Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO classification system (PALMCOEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive
age. FIGO Working Group on Menstrual Disorders. Int J Gynaecol Obstet 2011;113:3–
13.
29) ACOG Practice Bulletin on Diagnosis of Abnormal Uterine Bleeding in ReproductiveAged Women. Number 128, July 2012.Chapter 11: Ultrasound of the Non-Pregnant Uterus 252
30) N O’Connoll LP, Fries MH, Aeringue E, Brehm W. Triage of abnormal postmenopausal
bleeding: a comparison of endometrial biopsy and transvaginal sonohysterography versus
fractional curettage with hysteroscopy. Am J Obstet Gynecol 1998;178:956-61.
31) Schwarzler P, Concin H, Bosch H, Berlinger A, Wohlgenannt K, Collins WP, et al. An
evaluation of sonohysterography and diagnostic hysteroscopy for the assessment of
32) Kelekci S, Kaya E, Alan M, Alan Y, Bilge U, Mollamahmutoglu L. Comparison of
transvaginal sonography, saline infusion sonography, and office hysteronscopy in
reproductive-aged women with or without abnormal uterine bleeding. Fertil Steril
2005;84:682–6.
33) Soares SR, Barbosa dos Reis MM, Camargos AF, Diagnostic accuracy of
sonohysterography, transvaginal sonography, and hysterosalpingography in patients with
uterine cavity diseases. Fertil Steril 2000;73:406-11.
34) American Cancer Society: Cancer Facts and Figures 2008. Atlanta, Georgia ACS: 2008.
www.cancer.org/STT/2008CAFFFinalSecured.pdf
35) Goldstein RB, Bree RL, Benson CB, Benacerraf BR, Bloss JD, Carlos R et al. Evaluation
of the woman with postmenopausal bleeding. Society of Radiologists in UltrasoundSponsored consensus conference statement. J Ultrasound Med 2001;20:1025-36
36) Bakour SH, Khan KS, Gupta JK. Controlled analysis of factors associated with
insufficient samples on outpatient endometrial biopsy. BJOG 2000; 107:1312-4.
37) Fleischer AC, Wheeler JE, Lindsay I, Hendrix SL, Grabill S, Kravitz B. An assessment of
the value of ultrasonographic screening for endometrial disease in postmenopausal
women without symptoms. A J Obstet Gynecol 2001; 184:70-5.
38) Kwon JH, Kim GS. Obstetric iatrogenic arterial injuries of the uterus: diagnosis with US
and treatment with transcatheter arterial embolization. Radiographics 2002; 22:35–46.
39) Yahi-Mountasser H, Collinet P, Nayama M, Boukerrou M, Robert Y, Deruelle P. Les
malformations artério-veineuses intra-utérines. À propos de 4 cas. J Gynecol Obstet Biol
Reprod (Paris) 2006; 35:614–20.
40) Bauer V, Briex M, De Meeus JB, Drouineau J, Ferrie JC, Magnin G. Malformation
artérioveineuse congénitale de l’artère iliaque interne découverte au cours de la grossesse.
J Gynecol Obstet Biol Reprod (Paris) 1993; 22:312–6.
41) S. Sanguin, S. Lanta-Delmas, A. Le Blanche, E. Grardel-Chambenoit, P. Merviel, J.
Gondry, R. Fauvet. Diagnostic et traitement des malformations artério-veineuses utérines
(MAVU) en 2011
42) Timmerman D, Van Den Bosch T, Peeraer K, Debrouwere E, Van Schoubroeck D,
Stockx L, et al. Vascular malformations in the uterus: ultrasonographic diagnosis and
conservative management. Eur J Obstet Gynecol Reprod Biol 2000; 92:171–8.
43) Kwon JH, Kim GS,: Obstetric iatrogenic arterial injuries of the uterus: Diagnosis with US
and treatment with transcatheter arterial embolization. Radiographics 2002;22:35.
44) Delotte J, Chevallier P, Benoit B, Castillon JM, Bongain A. Pregnancy after embolization
therapy for uterine arteriovenous malformation. Fertil Steril 2006;85:228.
Nhận xét
Đăng nhận xét